The variant poliovirus strains detected in six wastewater samples, collected from two environmental surveillance sites in Khan Younis and Deir al Balah. Further genomic sequencing of poliovirus isolates has identified that these strains have close genetic links with each other and are also closely related to the poliovirus variant that was circulating in Egypt during the second half of 2023. The last detection of the related variant polioviruses in Egypt was in samples collected in December 2023. Based on the analysis of genetic changes in the isolates, the variant poliovirus could have been introduced in Gaza as early as September 2023. It is important to note that virus has been isolated from the environment only at this time; no associated paralytic cases have been detected.
A risk assessment is being implemented, led by the Ministry of Health, including to assess surveillance sensitivity for the detection of acute flaccid paralysis (AFP) and environmental surveillance, and subnational immunity levels are being more clearly assessed.
WHO, UNICEF and UNRWA continue to work with all public health authorities on the ground, as part of urgent efforts to mitigate the impact of the current crisis on the health of populations in Gaza. The ongoing crisis continues to pose a significant challenge to the ability to implement full disease surveillance and outreach with immunization services.
Routine immunization rates in the occupied Palestinian territory (oPt) were optimal before the start of conflict in October 2023. Polio vaccination coverage (POL3), primarily conducted through routine immunization, was estimated at 99% in 2022. This has declined to 89% in 2023, according to the latest WHO-UNICEF routine immunization estimates (WUENIC).
Currently, only 16 out of 36 hospitals are partially functional and 45 out of 105 primary health care facilities are operational. The impact on health system, insecurity, inaccessibility, population displacement, and shortages of medical supplies, coupled with poor quality of water and weakened sanitation, have contributed to reduced routine immunization rates and an increased risk of vaccine-preventable diseases, including polio.
WHO considers there to be a high risk of spread of this strain within Gaza, and internationally, particularly given the impact the current situation continues to have on public health services.
This statement was published on 19 July and was updated with additional information on 21 July.
On 14 May 2024, the wild poliovirus outbreak in Malawi and Mozambique – which paralyzed nine children across the countries between February and August 2022 – was officially stopped. The virus, linked to a strain originally found in Pakistan, was unable to regain a foothold in the African region.
This incredible achievement was made possible by the tireless efforts of health workers and authorities across five countries – Malawi, Mozambique, Tanzania, Zambia, and Zimbabwe. Over two years, with support from the Global Polio Eradication Initiative (GPEI), they reached more than 50 million children through massive, coordinated vaccination campaigns and set up 15 new wastewater surveillance sites to quickly detect and respond to any trace of polio.
But that wasn’t all. The gender norms, roles, and relationships that can impact a health worker’s ability to access every household and guide a family’s decision to vaccinate their child were considered every step of the way. From planning campaigns to dropping the vaccine in children’s mouths, acknowledging and addressing these nuances was key to ensuring that every child was protected from this devastating disease.
For example, in Malawi, the program partnered closely with the Ministry of Gender to use a new tool first deployed during the COVID-19 pandemic – the Rapid Gender Assessment Tool. This tool analyzes the different impacts a disease has on women and men, with a particular focus on disadvantaged groups like women living in rural areas, to ensure policies and interventions around outbreaks provide equal protection for all. The insights from this tool proved vital for the wild polio outbreak in southern Africa.
The Ministry of Gender and the GPEI employed a gender-specific approach to tackle cultural barriers hindering immunization access. This strategy, informed by the Rapid Gender Assessment Tool and COVID-19 data, addressed key gaps. This included ensuring plans considered the different needs and roles of men and women in the community and tracking immunization rates by gender to identify and address any disparities in reaching boys and girls.
Gender-balanced vaccination teams navigated local customs to ensure access to all households. Community meetings at markets, schools and local health facilities further fostered dialogue with both men and women, ensuring everyone was informed and empowered to participate in vaccination campaigns.
Recognizing the importance of a data-driven approach, the country team developed additional monitoring and reporting formats to improve data collection. These formats captured information on gender not only of children vaccinated but also of polio teams working at all levels including decision-making, campaign implementation, monitoring and supervision.
Approaches like these, with gender at the center, helped the program make significant strides against the virus across southern Africa.
Malawi, Mozambique, and many countries still battle another threat – variant poliovirus – and as long as any kind of polio exists, every child remains at risk. The tools and tactics used to respond to the wild polio outbreak will be invaluable as countries work to end all forms of the virus for good.
MONROVIA, Liberia, 04 June 2024 – Michael Essien, the celebrated football icon and coach, along with his wife, Akosua Puni Essien, are visiting Liberia to advocate for the eradication of polio. This visit aims to support the Liberian government’s ongoing efforts to eradicate polio, and increase child immunization, coinciding with the synchronized polio campaign across Liberia and six West African countries.
Liberia, having reported a resurgence of variant polio type 2 in wastewater, is now at the forefront of a critical fight against this disease. The nation has embarked on two rounds of nationwide immunization campaigns using the novel oral polio vaccine (nOPV2) to quickly stop the spread of the virus, with the second round set to begin on 7 June. While vaccine coverage rates are showing promising progress, the battle against polio requires unwavering commitment and action.
Mr. Adolphus Clark, Expanded Programme on Immunization (EPI) Manager in Liberia, has expressed his optimism about the campaign, stating, “Our collective efforts have brought us closer than ever to a polio-free Liberia. With the support of Michael and Akosua Essien and our global partners, we are renewing our commitment to ensure that every child is protected from this preventable disease.”
The campaign is one of hope and determination. Despite the challenges, the number of variant poliovirus cases has significantly declined, with no children paralyzed by polio since 2021. The focus remains on reaching zero cases and maintaining vigilance until polio is eradicated from the region and the world.
During their visit, the Essiens have engaged in a learning trip focused on immunization and polio eradication efforts in Liberia, understanding the vaccine infrastructure, and listening to personal stories from families and children receiving vaccines as well as the health care workers administering them. Michael also participated in a friendly football game with young athletes in Liberia.
Akosua Puni Essien has expressed her enthusiasm for the eradication efforts in Liberia, stating, “It is inspiring to see the coordinated efforts in Liberia to ensure every child receives vaccination to protect them from the polio virus. I urge all parents and caregivers to ensure that children under the age of five-years-old receive their vaccines – the polio vaccine is free, safe, and crucial for protecting our children from this devastating disease.”
The collective efforts of frontline workers, communities, local governments, Rotarians, and other global partners have been instrumental in the fight against polio in Liberia and worldwide. With continued dedication and support, the goal of eradicating polio in Liberia and Africa is within reach.
“Through unity and determination, most of the world has overcome the shadow of polio. Let its eradication be a beacon of hope, reminding us that with perseverance, even the most daunting challenges can be conquered,” said Michael Essien. “I am inspired by the tenacity of the Liberian people, and I know that together, we will finish the job so no child ever has to live in fear of polio again.”
The Essiens’ visit has been organized by the Gates Foundation and UNICEF, in coordination with the government of Liberia.
“The visit of Michael and Akosua Essien underscores the power of partnership in our fight against polio. Their presence boosts confidence in vaccination and highlights our shared commitment to a polio-free future for every child in West and Central Africa. Together, we can make polio history,” said Andy Brooks, UNICEF Representative in Liberia.
Notes to Editors
Photos from the visit are available upon request from: Mostafa Omar mosomar@unicef.org
Liberia Polio Situation
Liberia reported two variant polio type 2 detections from environmental sampling in 2023 and 6 so far in 2024. Environmental surveillance involves testing sewage or other environmental samples for the presence of poliovirus, often confirming it in the absence of clinical cases of paralysis. This comes after a period of almost two years without any detection of variant polio type 2 in Liberia. There have been no symptomatic cases in children since 2021. As a result, Liberia has been prioritized for 2 rounds of nationwide nOPV2 campaigns, with the first round implemented on 10 May synchronized with six West African countries and the second round scheduled to begin on 7 June.
Routine Immunization Overview in Liberia
Liberia has introduced seven vaccines into their routine immunization schedule: Pneumococcal Conjugate Vaccine (PCV), Rotavirus (RV), Inactive Polio Virus (IPV), Haemophilus Influenzae Tue B (HIB), Typhoid, and Measles containing vaccine (MCV2). Latest coverage rates from the 2023 WHO/UNICEF Estimates of National Immunization Coverage (WUENIC) data report range from 78% for HIB to 59% for MCV2. IPV coverage rates have recently improved from 66% in 2019 to 71% in 2022.
The President of the Republic of Madagascar, Andry Rajoelina, and the First Lady, Mialy Rajoelina, received a high-level delegation from the Global Polio Eradication Initiative (GPEI) on April 25, 2024 in Ambohitsorohitra palace in the capital, Antananarivo.
The delegation included the Regional Director of the World Health Organization (WHO) for Africa, Dr Matshidiso Moeti, the President of the Polio Oversight Board, Dr Chris Elias, the Regional Director of UNICEF for Eastern and Southern Africa, Etleva Kadilli, and the Director of Health Systems Strengthening and Immunization from Gavi, the Vaccine Alliance, Alex de Jonquieres.
To read more about the meeting, a press release is available here in French.
To strengthen the fight against polio, health ministers from across the WHO Eastern Mediterranean Region gathered virtually for the 10th meeting of the Regional Subcommittee on Polio Eradication and Outbreaks. It was the first meeting of the Subcommittee convened by the new WHO Regional Director for the Eastern Mediterranean, Dr Hanan Balhky.
Her Excellency Dr Hanan Al-Kuwari, Minister of Public Health, Qatar, and Subcommittee Co-chair, welcomed Dr Balhky’s determination to end polio during her tenure. His Excellency Mr Abdul Rahman Mohammed Al Oweis, Minister of Health and Prevention of the United Arab Emirates, and Subcommittee Co-chair, represented by His Excellency Dr Hussain Al Rand, also expressed enthusiasm that Dr Balkhy’s vision and expertise promise to propel regional efforts, bringing the world closer to eradication.
The stories below highlight some ways in which women are breaking barriers, driving change and inching us closer to a polio-free world wherever they take charge – from doorsteps to laboratories to decision-making tables.
Driving regional solidarity for polio eradication
Dr Hanan Balkhy, WHO Regional Director for the Eastern Mediterranean
Dr Hanan Balkhy made history in February 2024 when she became the first woman to take up the post of WHO Regional Director for the Eastern Mediterranean. With unwavering determination, she embarked on her new role with a clear vision: to eradicate polio during her tenure.
In her nomination speech, she shared her inspiration, drawn from success stories of joint efforts across the WHO Eastern Mediterranean Region. Dr Balkhy fervently believes in the need for collective action to overcome the obstacles in the path to polio eradication.
Dr Balkhy will convene the Regional Subcommittee for Polio Eradication and Outbreaks. To champion the Region’s work to consign polio to history, she will support the regional polio eradication programme, remove obstacles and work closely with global and regional decision-making bodies.
She calls upon all stakeholders to unite with resolute determination until polio becomes nothing more than a distant memory.
Blazing a trail with the Regional Subcommittee
Her Excellency Dr Hanan Mohamed Al Kuwari, Minister of Public Health, Qatar
An inspiration to women globally, Qatari Minister of Public Health H.E. Dr Hanan Mohamed Al Kuwari has been harnessing decision-makers’ power to galvanize action for polio eradication.
As Co-Chair of the Regional Subcommittee for Polio Eradication and Outbreaks since 2022, she has created a strong sense of solidarity among Member States of the Region and partners, reminding them of the urgent need to prioritize polio eradication. Using every possible chance to highlight the challenges faced by countries with wild or variant poliovirus cases, she has mobilized action to reach vulnerable children with polio vaccines and other health services.
Dr Al Kuwari has used her platform and voice to reveal issues faced by polio eradicators in the Region and offer solutions. At the same time, she has raised the visibility of the trailblazing Regional Subcommittee’s goals and work.
Economic and social benefits totalling an estimated US$ 289.2 billion arise from sustaining polio assets and integrating them into expanded immunization, surveillance and emergency response programmes in 8 countries of the Eastern Mediterranean Region, the study reveals. As the present cost of this work is US$ 7.5 billion, this means that for every dollar spent, the return on investment is nearly US$ 39.
WHO commissioned the Victoria Institute of Strategic Economic Studies, Australia, to conduct the study, which is the first of its kind. It covers 8 polio transition priority countries in the Region: Afghanistan, Iraq, Libya, Pakistan, Somalia, Sudan, Syria and Yemen. Many of these countries are fragile, with challenges ranging from weak health systems and low routine vaccination coverage to political instability.
Conflict could have the worst impact on vulnerable children, who are victims of circumstances beyond their control or capabilities. Almost a decade of conflict has led Yemen to experience devastating outbreaks of vaccine-preventable diseases, which disproportionately affect children. Key contributing factors include extremely limited public health infrastructure and services, limited water availability, and growing levels of vaccine denial and hesitancy.
“Children are particularly vulnerable to vaccine-preventable diseases such as polio, measles, pertussis and diphtheria,” said Dr Arturo Pesigan, WHO Representative and Head of Mission in Yemen. “One in 4 Yemeni children has not received all the recommended vaccinations on the national routine immunization schedule, and 17% are zero-dose children, who have not had a single dose of diphtheria-tetanus-pertussis vaccine.”
Geneva, Switzerland, January 2024 – Convening this week at the World Health Organization (WHO) headquarters, global health leaders and Ministers of Health at the WHO Executive Board (EB) reaffirmed their commitment to eradicate polio once and for all and use the polio investments to build strong, equitable and resilient health systems.
Opening the EB amid a wide array of public health topics on the agenda, WHO Director-General Dr Tedros Adhanom Ghebreyesus told assembled delegates: “We continue to intensify our efforts to eradicate polio. Last year, six cases of wild poliovirus were reported in Pakistan, and six in Afghanistan, the second-lowest number of cases reported in a calendar year. Our target is to interrupt transmission of wild poliovirus this year.”
Member States noted the unique opportunity to eradicate remaining wild poliovirus type 1 endemic transmission, which is now limited to just a handful of areas of eastern Afghanistan and three districts of southern Khyber Pakhtunkhwa, Pakistan, and urged for continued intensified efforts to reaching all remaining un- or under-immunized children in those areas. Delegates also reiterated the importance of intensifying efforts to combat variant poliovirus outbreaks (circulating vaccine-derived polioviruses), including through strengthened outbreak response and the continued roll-out of novel oral polio vaccine type 2, which became the first vaccine used under Emergency Use Listing (EUL) to be pre-qualified by WHO. The engines of transmission for such strains are in clearly-identified and known most consequential geographies, namely north-western Nigeria, eastern Democratic Republic of the Congo, south-central Somalia and northern Yemen.
Speaking on behalf of WHO Regional Director for the Eastern Mediterranean Dr Ahmed Al Mandhari, Dr Hamid Jafari, Director for Polio Eradication in the Eastern Mediterranean said: “In Afghanistan and Pakistan, the national programmes deployed innovative strategies and strengthened partnerships with humanitarian actors to reach more children. And across the region, the programme also identified pathways for sustaining essential polio functions, through integration with existing programmes. In particular, I am proud of the work of the Regional Subcommittee for Polio Eradication and Outbreaks that we started back in 2021. Their advocacy and support have successfully carved out clear pathways towards protecting children in the Region from polio and other vaccine-preventable diseases.”
Within this context, delegates thanked current Regional Director Dr Ahmed Al Mandhari, for his personal engagement and leadership in bringing the region to the threshold of success; and welcomed his successor, Dr Hanan H Balkhy, who committed to leading the region across the finish line.
“On behalf of the core partners of the Global Polio Eradication Initiative, Rotary International, the US Centers for Disease Control and Prevention (CDC), UNICEF, the Bill & Melinda Gates Foundation and Gavi, the Vaccine Alliance, we would like to thank all Member States for their tremendous efforts,” said Aidan O’Leary, WHO Director for Polio Eradication and Chair of the Global Polio Eradication Initiative Strategy Committee. “Last year, thanks to your efforts, upwards of 800 million children were immunized, many in areas with protracted and complex emergencies. The reality is that it is precisely in such areas of complex emergencies where polio persists, and unfortunately those emergencies are becoming even more complex. We need the continued political will of Member States to overcoming whatever geo-political challenges might currently stand in the way of reaching that remaining last unreached child in these areas. Be assured that together with our partners, we stand ready to support you in your incredible efforts.” Underscoring WHO’s commitment to the effort, O’Leary reminded the EB that WHO now considered the effort to eradicate polio as its only Public Health Emergency of International Concern (PHEIC), under the International Health Regulations (IHR).
O’Leary also reminded delegates of our collective duty to prepare for a lasting polio-free world. He referenced specifically the new approach to polio transition, which draws upon lessons-learned, and puts countries at the forefront, as solutions need to be country-specific, tailored to each country’s own context. Within that context, delegates emphasized the importance of implementing all activities to not only achieve a polio-free world, but also to sustain it through strengthening essential immunization, surveillance, integration and transition, reiterating their support and commitment to fully finance the Global Polio Eradication Initiative Strategy and the WHO base budget.
Speaking on behalf of Rotarians around the world and civil society as a whole, Judith Diment of Rotary International’s PolioPlus Committee, congratulated delegates on ongoing efforts to protect children from devastating diseases such as polio. “The Global Polio Eradication Initiative is closing in on zero, with fewer cases in fewer places in 2023, reaching more children through tailored approaches to increase public demand and identifying missed children. We applaud the use of targeted, integrated activities.”
The Global Polio Eradication Initiative has two goals laid out in its current strategy: to interrupt all remaining transmission of endemic wild poliovirus type 1 (WPV1) and to stop all outbreaks of variant poliovirus type 2 (cVDPV2). 2023 was a critical year for progressing on each of these, and while our urgent and diligent work to end polio must continue into 2024, the GPEI achieved incredible things in the past twelve months.
Continuing work in endemic countries
Despite significant geo-political and environmental challenges in the two remaining WPV1-endemic countries, Pakistan and Afghanistan, the polio programme has continued to reach greater numbers of children with polio vaccines.
Wild polio transmission was beaten back to just a handful of districts in eastern Afghanistan and the southern area of Khyber Pakhtunkhwa province in Pakistan. In both countries, efforts are increasingly focused on reaching and vaccinating the last remaining ‘zero dose’ children – children who have received no vaccines of any kind. The number of these missed children continues to dwindle, with the success of improved collaboration with the national immunisation program, new efforts like Pakistan’s Nomad Vaccination Initiative and focused vaccination activities at border crossings between the two countries. Just one family of the virus remains endemic in each country, and coupled with this increasing geographic restriction, the situation resembles the end of wild polio eradication efforts in former virus hotspots like India, Nigeria and Egypt.
In addition, after a wild poliovirus outbreak that was confirmed in southeast Africa in early 2022, neither Malawi nor Mozambique has reported a WPV case since August 2022 thanks to a concerted subregional emergency response across five neighbouring countries. We are hopeful that this outbreak will be officially closed in the coming months, affirming that countries have what it takes to protect children from this devastating disease and keep wild polio out of Africa.
Progress on variant polio outbreaks
Thanks to the novel oral polio vaccine type 2 (nOPV2), strong political commitment and community-based efforts to reach more children with the vaccine, the number of cases of variant poliovirus type 2 (cVDPV2) continued to decline in 2023.
Nearly 1 billion doses of nOPV2, a comparably safe, effective, but more genetically stable version of the existing type 2 oral polio vaccine (mOPV2), have now been administered across 35 countries, protecting millions of children from illness and paralysis.
Emergency response to variant polio outbreaks is continuing, notably in the most consequential geographies for the programme—where children are at the highest risk of encountering and spreading poliovirus. In northern Nigeria, for example, variant polio cases have fallen by 90% since a peak in 2021, thanks to concerted commitment from government, unique community programs to improve the reach of vaccines and the extensive rollout of nOPV2. Across these consequential geographies, the programme will continue to focus on increasing access, acceptance and campaign quality, which have helped make incredible progress in Nigeria, and continue to innovate until we end polio for good everywhere.
Finally, In September 2023, after a massive vaccination response in the shadow of ongoing war, Ukraine officially stopped its outbreak of type 2 variant polio that began in 2021. New York, London and Jerusalem, where high-profile outbreaks began in 2022, have not detected the virus in recent months. Still, the emergence of polio in these areas is a reminder that as long as poliovirus exists anywhere, it is a threat to people everywhere.
Most importantly, thanks to the efforts of the GPEI and its partners, health workers vaccinated more than 400 million children in 2023, preventing an estimated 650,000 cases of paralysis from polio and saving the lives of up to 60,000 children. Building full, healthy futures was at the core of Rotary International’s mission when it began this fight to end polio for good in 1985, and when the GPEI was launched in 1988—35 years ago.
This year, the Independent Monitoring Board (IMB) conducted a rigorous mid-term review of the GPEI’s progress towards its strategic goals. This welcome counsel is already helping inform and guide the GPEI’s own ongoing analysis and strengthening of its strategic approaches to achieve a polio-free world, as the programme published its initial response to the mid-term review, under the guidance of the Polio Oversight Board (POB).
Achieving and sustaining a polio-free world has proven harder – and taken longer – than anyone could have imagined. But making history is never easy, and we are confident that together we can eradicate a second human disease from this earth, and build stronger, more resilient health systems along the way.
2023 has firmly set the stage for success. With the complexities of the world today, this programme still inspires to bring about the very best in our humanity.
Thank you to all who have contributed to this effort so far and continue to do so. Let us double down and make the dream of a polio-free world a reality.
Nearly 1 billion people globally1 are served by health care facilities that do not have regular or consistent power. Unreliable energy disrupts routine and emergency care—from running diagnostic tests to ensuring vaccines stay cold. As heatwaves, floods, and other extreme weather events become more common, energy disruptions are expected to increase due to events like power outages and heat stress on existing infrastructure. To address these challenges in the last mile of polio eradication and reduce its carbon footprint, the GPEI and partners have turned to solar power, a more affordable, reliable and climate-resilient energy source to power polio vaccination and surveillance activities.
Solar powered vaccine refrigerators
For decades,2 refrigerators powered by fossil fuels like kerosene or petrol were essential to maintaining vaccines at just the right temperature. Yet, these refrigerators emitted greenhouse gases (GHGs), were relatively expensive to operate and were vulnerable to disruptions in the national energy supply. Now, the GPEI and its partners significantly rely on solar power, specifically, Solar Direct Drive (SDD) vaccine refrigerators.3 SDD refrigerators can run for days without power if needed, not only making them more dependable, but also extending the programme’s reach in some of the most difficult yet critical areas to end polio.
In the Democratic Republic of the Congo,4 a country the size of Western Europe with difficult terrain and longstanding security challenges, millions of children have missed out on polio and other life-saving vaccines in part because vaccines could not be kept cold on the trip to reach them. In 2016, just 16% of health centres in the country had a working refrigerator. Between 2018 and 2021, Gavi and its partners helped address this gap by delivering over 5,500 new solar-powered fridges across the country.
On the remote islands of Lake Chad,5 the introduction of solar powered refrigerators means that parents and health workers can simply go to the community center on the island, rather than travelling long distances by boat to receive or administer polio vaccines. Meanwhile, in Somalia, a country that experiences frequent interruptions in power supply, all vaccine refrigerators from the regional storage points down to the community-level administration are now powered by SDD refrigerators.
Solar powered surveillance
During surveillance, stool and environmental samples travel through the vaccine cold chain in reverse – from the field site or clinic to the regional and global laboratories for testing. In January 2021, an insurgency in Borno state, Nigeria, showed the world just how vital reliable, climate-resilient energy for surveillance is. The insurgency resulted in over ten months of power outages, including at the University of Maiduguri Teaching Hospital, which houses one of only two national polio laboratories in Nigeria. This meant that samples from the 10 most vulnerable states for polio transmission in northern Nigeria couldn’t be tested.
To help the lab get back on track as quickly as possible and prevent future power issues, the World Health Organization6 provided 48 solar panels. As a result, throughout most of 2021, more than 10,000 stool samples of children with acute flaccid paralysis (AFP) and more than 500 environmental samples were analyzed by the laboratory, an essential step to finding and stopping the virus.
In the face of the climate crisis and its many knock-on effects, including extreme weather events and even more persistent conflicts, health programmes like the GPEI must continue to integrate renewable energy at every turn. From refrigerators to powering entire laboratories, solar power technology has become a key energy source to help reduce the GPEI’s GHG emissions and ensure a polio-free future.
[1] Energizing health: accelerating electricity access in health-care facilities. Geneva: World Health Organization, the World Bank, Sustainable Energy for All and the International Renewable Energy Agency; 2023. Licence: CC BY-NC-SA 3.0 IGO [2] https://www.unicef.org/innovation/stories/using-sun-keep-vaccines-cool [3] https://apps.who.int/iris/bitstream/handle/10665/254715/WHO-IVB-17.01-eng.pdf;sequence=1 [4] https://www.gavi.org/vaccineswork/drcs-solar-revolution [5] https://archive.polioeradication.org/news-post/protecting-against-polio-in-lake-chad/ [6] https://www.afro.who.int/news/who-delivers-solar-panels-accredited-polio-laboratory-borno-state
Stopping any polio outbreak starts with vaccine procurement, transport by airplanes and trucks, distribution involving complex logistics, and eventually the oral administration of the vaccine by drops in the mouths of every eligible child.
However, there is another, lesser known but equally important process that must also take place to halt transmission of the poliovirus. It begins with a humble stool sample – a thumb-sized smudge of poop – taken from a child with acute flaccid paralysis (AFP), then delivered to the nearest laboratory that can test the sample specifically for poliovirus.
But nowhere in Yemen is there any such lab. So the long and arduous journey of any stool sample from a Yemeni child to a receiving lab can take up to several days – following an easterly route, to the neighboring country of Oman.
An explanation of how stool samples are transported over such a distance starts with why: monitoring children under 15 years of age for signs of AFP, which is the most common sign of poliovirus infection. The Global Polio Eradication Initiative has set a benchmark of at least three AFP cases per 100,000 children under 15 years of age, a standard that Yemen has consistently met, thanks to the effectiveness of its surveillance system. This achievement is all the more remarkable considering that Yemen is entering its ninth year of internal conflict, with resulting population displacements, widespread food and fuel shortages, and a devastated health system (in which only 46% of hospitals and health facilities are only partially functioning or completely out of service).
Antananarivo – Quality assurance surveyor Anja Mandimbisoa arrives at a random lot numerically selected, throws her pen in the air, and whichever house it is pointing at when it lands is the next on her evaluation list. With their consent, she then sits down with the family to verify whether the children in the household have the mark on their little fingers confirming they have been vaccinated against polio.
“The fact that it is a random selection provides a true picture of immunization coverage at the district level,” explains Mandimbisoa, one of 16 external Lot Quality Assurance Sampling (LQAS) surveyors trained by World Health Organization (WHO) in Analamanga region, Madagascar, to identify any missed children.
As the country concludes its third round of polio vaccinations this year, the response reflects that the job to end polio does not end with the conclusion of a vaccination round. Instead, it is the actions between rounds that make all the difference.
WHO/Europe has declared an outbreak of poliovirus in Ukraine, detected in October 2021, officially closed. The European Regional Commission for the Certification of Poliomyelitis Eradication endorsed the closure of the outbreak during its annual meeting on 8 September 2023. The country has achieved this milestone – stopping transmission of the virus that threatened the lives and futures of its children and preventing spread to other countries – in the face of the ongoing war.
The comprehensive outbreak response, initiated by the Ministry of Health of Ukraine in December 2021, faced multiple challenges since the end of February 2022, including massive population displacement, destruction of health-care infrastructure and disruption of logistical routes for medical product deliveries.
“Stopping the spread of poliovirus in the midst of a devastating war is a major achievement and a clear demonstration of the highest level of political commitment of the Government of Ukraine to the welfare of its population,” said Dr Hans Henri P. Kluge, WHO Regional Director for Europe.
“In the face of unprecedented challenges, the necessary steps taken by the Ministry of Health of Ukraine to prevent the spread of poliovirus within and beyond the borders of Ukraine are immensely commendable.”
The decision to close the outbreak was based on:
the recommendations of a poliovirus outbreak response assessment (OBRA) conducted by Global Polio Eradication Initiative (GPEI) partners, including WHO, in May 2023;
additional documentation provided by Ukraine in support of the ongoing surveillance, immunization and communication efforts since May; and
a comprehensive review of poliovirus surveillance and vaccination performance in the countries hosting the majority of the Ukrainian refugee population.
The outbreak was first detected in a young child in Ukraine in October 2021, following the importation of a poliovirus that had emerged in Pakistan and was previously detected in Tajikistan in 2021. A second child became paralysed in December 2021, and an additional 19 close contacts tested positive without developing symptoms.
“The Ministry of Health of Ukraine declared importation of this poliovirus a local public health emergency, and acted swiftly since its detection in close coordination with the global public health community,” said Dr Viktor Liashko, Minister of Health of Ukraine.
Dr Liashko continued, “The outbreak is now closed, but our work to prevent polio and other vaccine-preventable diseases in Ukraine continues despite all obstacles. As long as polio remains a threat globally, Ukraine will remain vulnerable. The Ministry of Health is committed to strengthening vaccine-preventable disease surveillance and working to achieve and sustain high routine immunization coverage nationwide to protect every child.”
What does it take to stop a polio outbreak?
In October 2021 the detection of poliovirus in Ukraine triggered the declaration of a public health emergency in affected oblasts, the creation of a response working group with technical support from GPEI and WHO specialists, and an immediate epidemiological investigation including contact tracing and environmental sampling at a summer camp, school and residences where the virus had been initially detected.
On 30 December 2021 the Ministry of Health approved an action plan in response to the outbreak that included, among other initiatives, an accelerated immunization catch-up campaign for children aged 6 months to 6 years who had not received the required doses through routine immunization.
The campaign began in mid-February 2022, but its scale and pace were significantly affected by the war in Ukraine. GPEI partners including WHO provided technical and operational support tailored to the context to build capacity and strengthen routine immunization services, disease surveillance, communication and transportation of samples to reference laboratories abroad.
Dr Jarno Habicht, WHO Representative in Ukraine, coordinated the WHO response within the country. “WHO and GPEI partners have been on the ground from day one, supporting Ukraine’s health authorities, medical and public-health professionals, laboratory staff, and communities to keep this virus from spreading,” he explained. “The excellent collaboration and perseverance of the local and international teams to protect children in the most difficult of circumstances has been truly inspiring.”
Despite the many challenges in implementing the national action plan for the outbreak response, no new detections of poliovirus were identified after December 2021. The OBRA conducted in May 2023 assessed the critical components of the outbreak response, such as the quality of surveillance (and thereby the risk of undetected poliovirus transmission), planning and coordination, the vaccination campaign, routine immunization performance, communication, and vaccine management. Based on the field assessment and review of the documentation, the OBRA concluded that poliovirus was no longer circulating in Ukraine.
The OBRA in Ukraine was followed by a comprehensive review of actions taken by Bulgaria, Czechia, Hungary, Poland, the Republic of Moldova, Romania and Slovakia. This was coordinated by WHO/Europe with financial support from the United States Agency for International Development (USAID).
The review assessed the actions to expand capacities to detect the virus, identify gaps in vaccination coverage and increase coverage of the local populations hosting Ukrainian refugees, and offer vaccination to refugees entering from Ukraine. This review, along with the additional information provided by Ukraine on actions implemented during the months following the OBRA, enabled WHO/Europe to declare the outbreak officially closed.
Mr Robb Butler, Director of the Division of Communicable Diseases, Environment and Health at WHO/Europe, stated, “Ukraine has been steadfast in recent years in its efforts to achieve and sustain high routine vaccination coverage, and within the realm of the European Immunization Agenda 2030, WHO/Europe will continue to support health authorities to prevent further outbreaks of vaccine-preventable diseases including polio, measles, diphtheria and many more.”
Mr Butler concluded, “Tremendous credit goes to the health professionals and parents who continue to make every effort to vaccinate children on schedule to protect them from the threat of polio and other diseases, even while navigating the daily realities and dangers of war.”
Geospatial Tracking Systems have a critical role to play in the monitoring of vaccination teams during polio outbreak response campaigns. With support from the World Health Organization (WHO) and the rest of the Global Polio Eradication Initiative (GPEI), the mobile application was most recently utilized in Brazzaville during a national vaccination campaign from June 9 to 11, 2023, led by Congo’s Ministry of Health. Read more on the WHO Afro website.
One of the first tasks they took on was to find ways to detect the possible spread of an outbreak of variant poliovirus that was confirmed in December 2022 after a paralysed child living near the border with Chad tested positive for the virus. Immediately after the start of the conflict, they worked to maintain the essential function of surveillance for acute flaccid paralysis (AFP) – the most common symptom of polio – in children.
Prioritizing essential polio functions
Much like a relay race, in AFP surveillance, speed and coordination are key. Once health teams find a child with AFP, the race begins. But emergencies often present additional hurdles. In one of the localities in Sudan’s White Nile state, Ahmed Masaood, a health worker, was tasked with collecting two stool samples from a child presenting with AFP. However, when the roads outside turned unsafe during Ahmed’s visit, he ended up having to seek refuge with the family he was visiting for two nights. As soon as he could, he rushed to the state cold room with his stool carrier to drop off the samples for storage until they could be tested.
The next lap of the race involves getting children’s stool samples to a WHO-accredited laboratory for testing. Due to the conflict, Sudan’s polio laboratory is not functioning, which meant the polio programme urgently needed to look for another laboratory to test stool samples to determine if children presenting with AFP had indeed been infected with poliovirus.
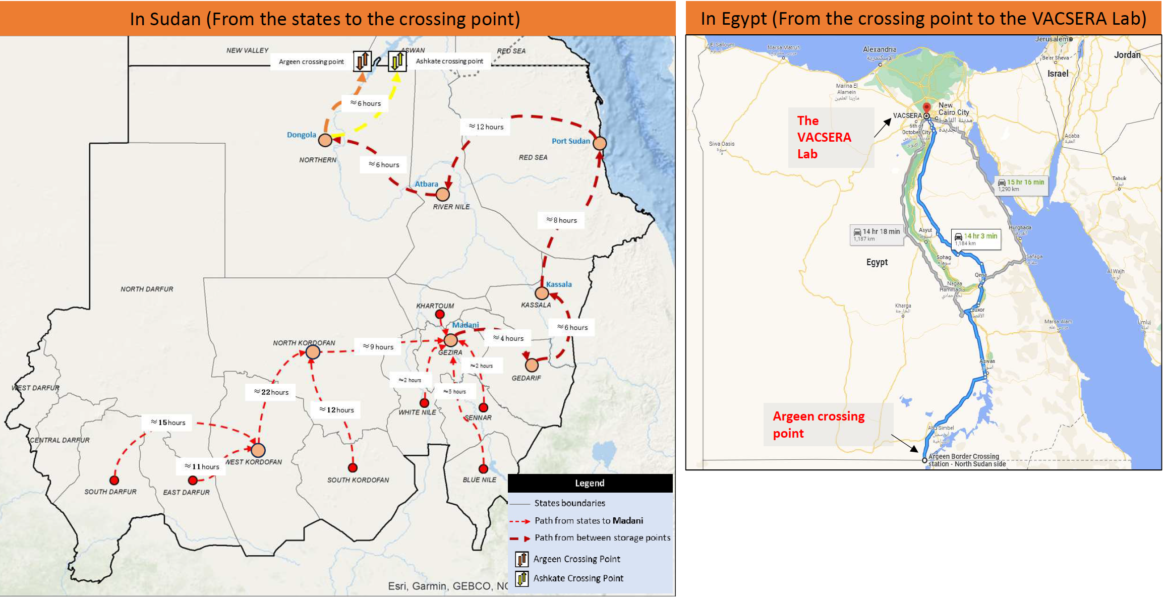
In a remarkable partnership, Sudan’s polio programme teamed up with Egypt’s health authorities to use the VACSERA laboratory in Giza for this crucial task. Senior decision makers at the Egyptian Ministry of Health not only approved the collaboration but instructed for it to begin as soon as possible.
In June, the polio programme in Sudan completed a pilot mission to transport stool samples to the VACSERA laboratory for testing. With the conflict impacting movement and security on the roads, creativity was required to get the samples from collection points identified, such as Gezira to Port Sudan to Dongola, all the way to the border. Throughout, health workers relied on two criteria to ensure safe passage for themselves and their cargo: first, their neutrality, and second, their status in communities. The health workers who made this happen are known to and trusted by the communities they serve, and that trust, in many cases built over decades, facilitated their travel by road.
The first shipment of stool carriers passed through five stops in different states following a pathway assessed for security considerations. In Red Sea state, Dr Thabit Mohammed Elsadig, a WHO Public Health Officer, spent three days pulling together all the resources drivers would need, from permits and security clearances to cash, fuel and food. As the situation was formally graded as a level three emergency, this triggered WHO’s Emergency Response Procedures, effectively enabling staff to respond and repurpose resources at speed. In some cases, Dr Thabit and others used their own resources to make things happen.
At each stop, health workers picked up more stool samplesfrom their colleagues. They checkedtemperature controls in the sample carrier and replaced old ice packs with fresh ones to maintaintemperature and handling protocols of the reverse cold chain.
With the occupation of the National Public Health Lab in Khartoum by one of the parties, Hatim Babiker Othman, National Coordinator for the Polio Lab in Sudan, moved to Port Sudan during the first month of the conflict and started to restructure the polio lab’s functions. He organized samples in small boxes, assigned lab numbers, and established effective communication with the focal point in Egypt, to coordinate the handover of samples. Hatim traveled with the samples from Port Sudan to Atbara, Dongola, and finally, the Argeen border crossing point.
Meanwhile, WHO colleagues contacted the Egyptian Ministry of Health to confirm that, at last, the samples were on their way to the border. At the Argeen Gate, border officials examined the boxes and their contents. Dr Thabit recalled thinking that if anything went wrong at this point, all their efforts – days of planning and transport by road – would have gone to waste.
“The sample carriers were like trunks of gold for us. We hoped they would treat them well, and they did,” he said, with reference to their value in signaling any epidemiological developments related to the ongoing variant poliovirus outbreak.
Exemplary inter-country support
Once they received a prompt from WHO, a team from Egypt’s Aswan Governorate of Health set out on a six-hour journey to the shared border. There, they collected the samples and headed back to the health facility in Aswan for more fresh ice packs before driving to the VACSERA laboratory in Giza, a 14-hour drive away. The entire journey from Madani, Sudan, to Giza, Egypt, can take up to 56 hours and demands absolute precision in planning and execution.
Acknowledging Egypt’s generous support, Dr Ni’ma Saeed Abid, WHO’s Representative in Sudan said, “Our partners in Egypt have demonstrated how stronginter-country collaboration can help in ending diseases. We remain grateful to them for their timely support, and to every link in this chain of coordination. This support is a demonstration of ‘delivering as one WHO’.”
On 16 June 2023, VACSERA received a shipment of 56 stool samples for testing for poliovirus.Lab personnel prioritized Sudan’s samples for immediate testing, and the testing process began on the day of arrival.Final results were shared in 11 days — a full 10 days less than the standard three weeks. The results were also good news: no sample tested positive for variant poliovirus.
“Our heroic health workers stayed to deliver our mandate and support the most vulnerable communities in the face of the ongoing conflict,” Dr Nima said. “They are continuously finding extraordinary solutions to continue to protect children from polio and other vaccine-preventable diseases. This is a lesson to be followed by the integrated disease surveillance team. It reinforces what we believe in:everything is possible, with strong determination and will.”
With 117 confirmed cases of circulating variant polioviruses and 107 detections in sampled wastewater so far in the African Region in 2023, the Africa Regional Certification Commission (ARCC) has urged countries and health partners to urgently address gaps in polio immunity to avert outbreaks.
The ARCC, which held it 31st meeting in the Democratic Republic of the Congo from 3 to 7 July, also called for an accelerate implementation of supplementary immunization activities, while considering challenges in accessibility to services including gender-related issues. The commission stressed the importance of gender equality in the polio fight, noting the crucial role women play in management, supervision, decision-making, message development and monitoring for polio control. The ARCC also urged countries to conduct robust preparations and ensure the vaccination campaigns are of the highest quality.
“The guidance will allow health authorities and partners to provide focused support to strengthen microplanning and social mobilization in areas with poor campaign performance, among other key areas of action“ said Professor Rose Leke, head of the Africa Regional Certification Commission.
The meeting gathered representatives of national and provincial health authorities from Chad, the Democratic Republic of the Congo, Ethiopia, Madagascar, Mali and Mozambique who committed to strengthen disease surveillance and consolidate the Expanded Programme on Immunization in hard-to-reach areas, with the support of the World Health Organization (WHO) and health partners.
Attendees took note of the increasing risk of poliovirus type 1 beyond Madagascar and the DRC, especially with the deterioration of routine immunization during the COVID-19 pandemic. Concerns were also raised regarding the persistently security-compromised areas, especially in Nigeria, that are impeding the elimination of circulating variant poliovirus type 2 (cVDPV2).
The commission, therefore, encouraged health authorities to also expand the use of Geospatial Information Systems to improve quality of surveillance and outbreak response.
“We are looking forward to implementing the additional ARCC recommendations to guide how we can deliver on the promise of polio-free Democratic Republic of the Congo and Africa,” said Dr Serge Emmanuel Holenn, Deputy Minister of Health of the Democratic Republic of the Congo, who applauded the commission, WHO and the Global Polio Eradication Initiative partners for the continued financial and technical support in the fight against polio in the country.
In addition to the DRC, Chad, Ethiopia, Madagascar, Mali and Mozambique also presented progress in polio control and lessons learned. Although certification of polio eradication occurs at the regional level, all countries with polio-free status are required to provide the certification commission with annual updates. These containment reports and outbreak preparedness plans allow for continuous monitoring.
The ARCC commended health authorities for their leadership in responding to ongoing polio outbreaks, as “this reflects the deep commitment and continued collective efforts by African countries and partner organizations to the fight against polio,” said Professor Leke.
The ARCC is an independent body established in 1998 to oversee the certification status of the African region as free from indigenous wild poliovirus. It continues to evaluate reliability of data in documentation submitted by National Certification Committees to ensure that countries are adhering to the criteria set for the global certification of wild polio virus. The ARCC meets twice a year to review progress made in the annual certification updates of selected countries on polio eradication activities of all the 47 member’s state of the WHO African region.
Global leaders and stakeholders have been unanimously declaring their solidarity to achieving a lasting world free of all forms of polioviruses.
Convening this week at the World Health Assembly in Geneva, Switzerland, Ministers of Health from around the globe evaluated the unique epidemiological opportunity which currently exists, in particular in eradicating all remaining chains of endemic wild poliovirus in a handful of districts of just two countries – Pakistan and Afghanistan. As a record number of Member States and civil society partners took to the floor, key to success, all experts agreed, must be on adapting operations and reaching remaining un- or under-immunized children in just seven subnational most consequential geographies, with collectively account for 90% of all new polio cases, including in a gender-equitable and integrated manner. To ensure lasting success, delegates urged country-specific solutions for polio transition. In response to both a wild poliovirus outbreak in south-eastern Africa and multi-country circulating vaccine-derived poliovirus outbreaks, extraordinary special sessions were led by WHO and its Regional Office for Africa between affected Member States and partners, to discuss concrete steps to stopping all outbreaks affecting the Region by end of year.
The World Health Assembly comes on the heels of last week’s G7 Leaders and G7 Health Ministers meetings in Japan, where both meetings highlighted the urgent need to ensure a world free of polio can be rapidly achieved. Next week, Rotarians from around the world are convening at the Rotary International Convention in Melbourne, Australia, to ensure civil society support for the effort will go hand-in-hand with public sector engagement.
Speaking on behalf of both Pakistan and the entire Eastern Mediterranean, Mr A.Q. Patel, Pakistan Federal Minister for National Health Services, Regulations and Coordination, said: “We are in the final leg of eradication and we are doing everything we have to do to achieve success. The virus is restricted to its smallest-ever geographical footprint, and the (polio) programmes in both Pakistan and Afghanistan continue to vastly expand their hunt for the virus and mount robust campaigns to reach all children, not just with polio vaccine, but indeed other antigens as well. We could not have come this far without the strong support and goodwill of all Member States, however there is still more to be done at the heart of all our work, and for the future of all generations of children. We need continued and sustained financial and political support from all Member States and partners, in order to give every child, no matter where they live, the promise of a polio-free world.”
H.E. Dr Hanan Mohammad Al-Kuwari, Minister of Public Health of Qatar, and Co-Chair of the Eastern Mediterranean Regional Subcommittee for Polio Eradication and Outbreaks, commented: “In our Region, we have made significant progress in both containing the spread of wild poliovirus and closing outbreaks of vaccine variant polio. Afghanistan and Pakistan have restricted the virus to the smallest geographical footprint in history and are now doubling up efforts to fully interrupt the remaining transmission. The engines fueling this progress are manifold, but the two most powerful, and the two I truly believe will get us across the line, are improved immunity and better surveillance. We are reaching and vaccinating more children, more often, and we are using the most sensitive and robust surveillance measures in history to ensure that if the virus is there, we are not missing it. Excellencies, partners and colleagues, I ask this as clearly as I can: Stay the course. Dig deep to do what needs to be done. Stand with us and be part of history.”
Noting the global commitments being made, Jean-Luc Perrin, Rotary International’s Representative to the United Nations in Geneva, told the global health community at the Assembly: “Polio eradication is a rare example of enduring, truly global collaboration toward a goal whose achievement will benefit all nations in perpetuity, while contributing toward broader global health priorities. We cannot take progress or possible victory for granted. Let us make collective history and End Polio Now!”
In conclusion: global leaders continue to note the very real window of opportunity for success this year, but that this window will not remain open for long. The virus will again gain in strength. Only collective and global collaboration will result in ultimate success, and delegates and leaders urge all stakeholders to keep the focus firmly on one overriding objective: reaching remaining un- or under-vaccinated children in the most consequential geographies. A collective responsibility, but if achieved, will result in success in 2023.
Additional quotes from the World Health Assembly:
“WHO and our partners remain steadfastly committed to finishing the job of consigning polio to history. Last year, three million children previously inaccessible in Afghanistan received polio vaccines for the first time. And in October, donors pledged US$2.6 billion to support the push for eradication. At the same time, as part of the polio transition, more than 50 countries have integrated polio assets to support immunization, disease detection and emergency response. We must make sure that the significant investments in polio eradication do not die with polio, but are used to build the health systems to deliver the services that these communities so badly need.”- Dr Tedros Adhanom Ghebreyesus, Director-General, World Health Organization
“Wild poliovirus transmission has been cornered to the smallest ever geographic locations in the Eastern Region of Afghanistan and seven districts in southern part of Khyber Pakhtunkhwa in Pakistan. However, the last 100-metre dash presents its own challenges and we must do all we can to achieve success.” Dr Hamid Jafari, Director for Polio Eradication for the Eastern Mediterranean, on behalf of Dr Ahmed Al-Mandhari, Regional Director, World Health Organization Eastern Mediterranean Region
“The African Region, which was certified free of wild poliovirus in 2020, has set itself the objective of stopping the transmission of all types of 2 polioviruses by the end of 2023 and integrating polio assets into activities that strengthen broader disease surveillance. It is also deploying integrated public health teams to respond to other emergencies, building on experiences from past poliovirus outbreaks and leveraging the polio network and infrastructure for response activities.” – Delegation of Burkina Faso, speaking on behalf of the entire African Region.
A key priority in 2023 is to end both wild- and variant polio transmission around the world is focusing on the most consequential geographies where children are at the highest risk of encountering and spreading the virus, and which collectively accounted for 90% of all new polio cases worldwide in 2022. Northern Nigeria is one of these seven subnational areas that now hold the key to a polio-free world.
In Nigeria increased vaccination and surveillance efforts have yielded positive results in 2022: No isolates from the country’s main historical transmission chain, the Jigawa lineage, which was responsible for most cases and international spread to many neighbouring countries in West Africa, have been detected since February 2022. There was a decline from 1028 cases as on 31st December 2021 to 168 cases as on the 31st December 2022. As a result, the virus is currently confined primarily to two states in the northwest zone of the country, namely Sokoto and Zamfara. This presents a distinctive opportunity for Nigeria to interrupt transmission by December 2023, according to the Expert Review Committee for Polio Eradication and Routine Immunization (ERC), the independent technical group advising the country on its eradication efforts.
In February 2023, the ERC convened its 39th meeting in Nigeria to make recommendations aimed at interrupting transmission of variant type 2 polio and maintaining its indigenous wild poliovirus-free certification status along with the entire African Region. Led by the Ministry of Health’s National Primary Healthcare Development Agency and supported by GPEI partners, Nigerian civil society and Rotarians across the country, efforts are intensifying to fully implement the National Polio Emergency Action Plan (NPEAP).
The country has developed a comprehensive National Polio Emergency Action Plan (NPEAP) to address the risks of all poliovirus types in order to ensure Nigeria and the entire Region’s certification status is maintained, within the context of the political transitioning process, the impact of COVID-19 on the national health systems and economy as well as the increasing concerns of insecurity affecting surveillance and vaccination reach. All recommendations made by the ERC are aimed at aligning the NPEAP with the 2022-2026 Global Polio Eradication Initiative (GPEI) Polio Eradication Strategy.
The ERC noted that the proposed activities for 2023 are contingent on three critical enablers, namely the global stockpile of novel oral polio vaccines (nOPV2) and bivalent oral polio vaccines (bOPV), constraints in financial resources, and a smooth political transition to drive political commitments at sub-national levels. Given the impact of variant type 2 poliovirus over the last few years, there should be limited room for complacency to reach the finish line for the interruption of these strains. The ERC, therefore, called on all partners to support the implementation of the NPEAP for 2023.
The conference also highlighted some of the achievements made in the fight against polio in Nigeria. The conference also highlighted some of the achievements made in the fight against polio in Nigeria. In 2022, there was an 84% decline in variant type 2 poliovirus cases, reduced from 415 cases in 2021 to 48 in 2022. The quality of Supplemental Immunization Activities (SIAs) improved, especially in the last quarter of 2022, and there were narrowed surveillance gaps at sub-national levels. Routine immunization (RI) coverage also improved from 33% in 2016 to 57% in 2022, and COVID-19 vaccination was also optimized to improve demand generation and delivery of other essential immunization vaccines.
The ERC made recommendations in nine thematic areas to fully implement the National Polio Emergency Action Plan, including by continuing to strengthen surveillance, mitigate risks due to inaccessibility and insecurity, build a more resilient routine immunization programme, assure solid vaccine management and advocate for a polio-free Nigeria.
In conclusion, 2023 is a critical year for polio eradication efforts in northern Nigeria and the other most consequential geographies for poliovirus transmission. The global community must continue to support these efforts to ensure that no child is left behind, and we can finally achieve a polio-free world.
The meeting came at a time of contrasts for polio eradication efforts. On the one hand, the Region’s most recent case of wild poliovirus was reported almost 5 months ago, in Pakistan, and the footprint of the virus is the smallest it has ever been. Additionally, efforts to search for polioviruses have never been stronger and the polio programme has made significant progress in accessing under-immunized children across a number of high-risk countries in the last year. On the other hand, the Region hosts 4 of the world’s 7 ‘consequential geographies’ – low-resource, high-risk areas in Afghanistan, Pakistan, Somalia and Yemen that the programme has identified as carrying a significant risk of spread of polio.
WHO’s Regional Director for the Eastern Mediterranean Dr Ahmed Al-Mandhari, who convened this virtual meeting, set the tone for the event by coining 2023 as a “defining year” for polio eradication.
He urged all Member States and partners to leverage the opportunity and momentum of the current moment and scale up collective efforts to wipe out polio. “Going forward, our regional solidarity and concerted action will be even more important, as we move closer to making history and ending polio,” said Dr Al-Mandhari.
Leading the demonstration of regional support to polio were the Co-chairs, Minister of Public Health of Qatar, HE Dr Hanan Al Kuwari, and Minister of Health and Prevention United Arab Emirates, HE Mr Abdul Rahman Mohammed Al Owais. They urged participating Member States to strengthen routine immunization and consider polio as “all of our problem” until transmission ends everywhere. They also called on Member States to offer all they can – funding, advocacy or technical expertise – to reach every child with vaccines.
Participants at the meeting also included ministers of health and senior delegates from countries in the Region, in addition to representatives from the Bill & Melinda Gates Foundation (BMGF), the Centers for Disease Prevention and Control (CDC), Gavi, Rotary and UNICEF.
In his address, the Minister of National Health Services Regulations and Coordination of Pakistan updated the audience of the timely and robust programmatic actions the country has been taking to end polio. In the face of catastrophic floods, the country turned response efforts into an opportunity to offer polio vaccines to children wherever possible. Additionally, Pakistan is using creative ways, such as truck art, to reach out to vulnerable communities living in hard-to-reach areas.
During discussions, the delegate from Egypt and the Minister of Health of Yemen offered updates on their polio eradication efforts, while delegates from Iraq and Saudi Arabia proposed actions to prevent the spread of polio during mass religious gatherings in their countries.
Member States and partners acknowledged the immense efforts directed at ending polio in the 2 countries where it is still endemic – Afghanistan and Pakistan – particularly in the wake of the earthquake and catastrophic flooding that took place in 2022, and the extraordinary political will and engagement in both countries. They also noted the work ongoing in countries witnessing outbreaks of circulating vaccine-derived poliovirus type 2 (cVDPV2), and lauded health workers for their valour and dedication to their work.
Member States also reiterated the importance of focusing on zero-dose children, and strengthening routine immunization and surveillance in countries that are polio-free and those that currently have polioviruses. They also commended Regional Director Dr Al-Mandhari for his leadership and requested him to continue to support Member States in the Region to push towards ending polio and attaining Health for All by All.
While updating participants on a recent visit made by a high-level mission to Pakistan last year, a representative from the BMGF, on behalf of Dr Chris Elias, the Chair of the Polio Oversight Board, acknowledged the extraordinary and unmatched efforts made in Pakistan by the political and health leadership, law enforcement and security agencies, to prevent any further spread of polio. Despite the flooding and political changes the country has faced, the polio programme continued to “shift gears” and mount a swift and robust response to polio. This was one of several visits that high-level missions have been making to Pakistan in support of eradication efforts.
In closing remarks, WHO representatives recognized Iraq and Syria for the strides both countries have taken to maintain essential polio functions, including in polio surveillance, while concurrently transitioning away from funding from the Global Polio Eradication Initiative.
The seventh meeting of the Regional Subcommittee for Polio Eradication and Outbreaks demonstrated the high level of confidence that Member States and partners have in the 2 remaining polio-endemic countries, Afghanistan and Pakistan. As polio remains a Public Health Emergency of International Concern under the International Health Regulations (2005), the intensified regional- and international-level collaboration of Member States and partners at events like this will serve as a springboard for focused action in 2023.
Note for editors
The Polio Oversight Board is the highest decision-making body in the Global Polio Eradication Initiative (GPEI). It brings together senior leadership of the 6 GPEI partner agencies—the Bill & Melinda Gates Foundation (BMGF), U.S. Centers for Disease Control and Prevention (CDC), Gavi, Rotary International, UNICEF, and the World Health Organization (WHO)—along with a representative of the GPEI’s donor community.
Dr Tedros Adhanom Ghebreyesus, Director-General of WHO, visited Pakistan in his role as Chair of the Polio Oversight Board at the time. Following this, since mid-2021, the Polio Oversight Board* made 3 visits, and Mr Bill Gates of the BMGF visited in February 2022.
Acknowledging that our common goal is to attain ‘Health for All by All’, which is a call for solidarity and action among all stakeholders;
Noting the progress achieved globally in eradicating poliovirus transmission since 1988;
Noting with deep concern the challenges involved in stopping ongoing outbreaks of circulating vaccine-derived poliovirus type 2 (cVDPV2) in the Region, without full access to vaccinate all vulnerable children in the affected populations;
Observing with alarm the prolonged outbreak in Yemen and the persistent restrictions on implementing outbreak response vaccination in the country’s northern governorates, and further observing that the cVDPV2 outbreak which has been continuing since 2017 is the world’s longest ongoing such outbreak;
Recognizing the Global Polio Eradication Initiative’s efforts to target its resources in the most impactful way by identifying particular areas affected by polio, including Yemen’s northern governorates and south-central Somalia, as “consequential geographies” – two of seven subnational geographies globally which together accounted for 90% of all polio cases in 2022 and which are all affected by broader humanitarian emergencies;
Recognizing the high risk of expansion of the polio outbreaks within and from the two Regional consequential geographies due to their complex emergency settings, limited access to high-risk populations, weak immunization services, gaps in coverage of supplementary vaccination campaigns, and unmitigated spread of misinformation and disinformation in northern governorates of Yemen;
Recalling that the international spread of polio is a Public Health Emergency of International Concern under the International Health Regulations (2005);
Observing with alarm that 197 children have been paralyzed by cVDPV2 in Yemen’s northern governorates, representing almost one-third of all global cases of this strain in 2022, and that the international spread of poliovirus from Yemen to Djibouti, Egypt and Somalia has been confirmed;
Recognizing the best operational approach and experience to vaccinate all children, especially infants and young children, against polio, and achieve more than 90% coverage to stop an outbreak is through house-to-house delivery of vaccination; and if that is not possible, to implement an intensified fixed site vaccination with effective mobilization of families and young children to fixed sites near their homes;
Recognizing the continued threat to all children posed by vaccine-derived poliovirus and the importance of regional solidarity and support to deliver on the goals of the 2022-2026 Polio Eradication Strategy, which have been endorsed and supported by a wide range of committed donors, such as Rotary International and Member States of the Region, in particular the UAE through the sustained commitment of His Highness Sheikh Mohamed bin Zayed Al Nahyan, President of the UAE;
We, the Member States of the Regional Subcommittee on Polio Eradication and Outbreaks for the Eastern Mediterranean:
DECLARE THAT:
The ongoing circulation of any strain of poliovirus in the Region is a Regional Public Health Emergency;
COMMIT TO:
Mobilizing all needed engagement and support by all political, community and civil society leaders and sectors at all levels to successfully end polio as a Regional Public Health Emergency;
Advocating with relevant community and subnational leaders to increase access and ensure full implementation of polio outbreak response in the most programmatically and epidemiologically impactful operational manner, ideally through house-to-house vaccination campaigns in all areas;
Focusing efforts on reaching remaining zero-dose children in the consequential geographies of the northern governorates of Yemen and south-central Somalia, working in the broader humanitarian emergency response context;
Helping to mobilize needed resources and highest-level international commitment to finalize and fully implement the Somalia Polio Eradication Action Plan 2023, in the context of competing health response priorities such as ongoing drought and the effects of the COVID-19 pandemic;
Helping to mobilize resources for the Global Polio Eradication Initiative partners to support the outbreak response in Yemen; and
Helping to strengthen coordination with other public health and humanitarian efforts in Somalia and Yemen, to ensure closer integration in particular with routine immunization and the delivery of essential health and nutrition services to children;
REQUEST THAT:
The international humanitarian and development communities scale up their support for providing essential services, including a robust vaccination response to the polio outbreaks in Somalia and Yemen using modalities that will deliver an acceptable level of coverage;
The authorities and polio eradication partners in Somalia accelerate high-quality and rigorous implementation of the Somalia Polio Eradication Action Plan 2023 to stop the longest-running outbreak in the country and prevent the further spread of cVDPV2 by the end of 2023;
10. The national authorities and the Regional Polio Eradication programme strengthen cross-border coordination across Somalia, Kenya, Ethiopia, Yemen and Djibouti, considering the documented importation of cVDPV2 from Somalia into Kenya and Ethiopia, and from Yemen into Djibouti, Egypt and Somalia, and the high risk of further instances of cVDPV2 crossing international borders;
11. Authorities in northern governorates of Yemen, all immunization partners and the humanitarian development community respond urgently to the unmitigated vaccine-related misinformation and disinformation that is being disseminated, which is risking the lives of thousands of children in Yemen and across the Region;
12. All authorities in northern governorates in Yemen facilitate the resumption of house-to-house vaccination campaigns in all areas to ensure the delivery of vaccines to the youngest and most vulnerable children, and in areas where house-to-house vaccination is not feasible, make all efforts to implement intensified fixed-site vaccination through a modality that also includes robust social mobilization and outreach to ensure high coverage; and
13. The Regional Director continue his strong leadership and efforts to support the cessation of polio outbreaks in Somalia and Yemen, including by advocating for all necessary financial and technical support, reviewing progress, implementing corrective actions as necessary, and regularly informing Member States of the aforementioned and of any eventual further action required, through the World Health Organization’s Executive Board, the World Health Assembly and the Regional Committee for the Eastern Mediterranean.
WHO/Bruno Pereira
Under the leadership of the Ministry of Health, with support from Rotary and other GPEI partners, a multi-round polio vaccination campaign is being implemented in Mozambique. Six rounds of vaccination were completed in 2022, covering all provinces of the country and reaching 8.7 million children.
A further four rounds of vaccination are planned for 2023. Rotary and GPEI partners are jointly working together to support health authorities to deliver training on community-based surveillance, procuring and distributing 30 million vaccine doses and 8000 vaccine carriers, expanding field surveillance efforts, supporting vaccine management and social behaviour change activities. The GPEI are also supporting the deployment of vaccination teams, under the overall coordination of the Ministry of Health.
During a visit to Mozambique from 21 to 23 February 2023, representatives of the United Nations Children’s Fund (UNICEF), World Health Organization (WHO), Bill & Melinda Gates Foundation, Rotary Foundation and the United States Centers for Disease Control and Prevention, emphasized the importance of building on lessons learnt and successful approaches used in polio eradication to strengthen the country’s response to other health emergencies, including the ongoing cholera outbreak.
The polio outbreak response in Mozambique comes as the country is also addressing other emergencies, including the COVID-19 pandemic, cholera, floods and insecurity in the northern Cabo Delgado region.
The senior leaders included UNICEF Regional Director for Eastern and Southern Africa, Mr Mohamed Fall, WHO Regional Director for Arica, Dr Matshidiso Moeti, Mr Chris Elias, the Chair of the Polio Oversight Board of the Global Polio Eradication Initiative (GPEI), Mr Mike McGovern, Chair of the Rotary International PolioPlus Committee, Dr Omotayo Bolu, Polio Eradication Branch Chief for the United States Centers for Disease Control and Prevention, and other partners.
They met with Mozambican Prime Minister Adriano Afonso Maleiane and visited Mozambique’s northern Tete province, where eight wild poliovirus cases were detected last year.
During their visit to Tete province, the delegation witnessed polio response efforts in the field, engaged with health workers and support staff, supervisors, religious and community leaders. They also visited an Emergency Operations Centre and a Cholera Treatment Centre to better understand challenges and progress in the polio and cholera responses.
“The Government of Mozambique has shown strong leadership in the response to polio, ensuring that all eligible children are reached and protected with the vaccine through effective immunization campaigns,” said Dr Moeti. “We must not relent nor spare efforts to finish the job of ending polio once and for all.”
Polio, a debilitating viral disease that was once the leading cause of paralysis among children worldwide, is very close to being eradicated. Since 1988, the number of children affected by polio has reduced by 99 per cent. But outbreaks continue to occur, including in Mozambique, and ensuring every last child is immunised against the virus is a global priority.
A total of nine wild poliovirus cases have been reported so far, with one in Malawi and eight in neighbouring Mozambique since the declaration of an outbreak on 17 February 2022 in Malawi. The last confirmed case to date was in August 2022 in Mozambique. The wild poliovirus in Malawi and Mozambique originated from Pakistan, one of the two last endemic countries.
Concerted emergency response launched following the outbreak in 2022 has helped increase protection among children through vaccines in Malawi, Mozambique, Zambia, Tanzania and Zimbabwe. The countries have also ramped up disease surveillance and community mobilization to help find cases and halt the virus.
“Southern Africa countries have made huge efforts to bolster polio detection, curb the spread of the virus and ensure that children live without the risk of infection and lifelong paralysis,” said Dr Matshidiso Moeti, World Health Organization (WHO) Regional Director for Africa. “We continue to support the polio control efforts across the region so that every child receives the protection they need.”
To date, 19 vaccination rounds have been concluded in the most at-risk areas and at least five more are planned for 2023 in the five countries.
Additionally, more than 10 new environmental surveillance sites have been set up over the past year in the affected countries with support from WHO. The fully operational sites are playing a critical role in the efforts to detect silent circulating poliovirus in wastewater.
“Response teams have worked intensely in the fight against polio not only in Malawi but in the rest of the neighbouring countries in a coordinated manner. We will not rest until we reach and vaccinate every child to stop polio transmission,” said Dr Emeka Agbo, acting Country Coordinator for the Global Polio Eradication Initiative in Malawi.
Reaching all households where eligible children live is critical to protect them against the risk of paralysis. The national health authorities, with support from the Global Polio Eradication Initiative, efforts are ongoing to map cross-border communities, migratory routes, border crossings and transit routes.
“Community health workers have been pivotal in the vaccination campaigns and will continue going door-to-door, bringing polio vaccines to children who might otherwise be missed,” said Dr Jamal Ahmed, WHO Polio Eradication Programme Manager.
Polio is highly infectious and affects unimmunized or under immunized children. In Malawi and Mozambique, it has paralysed children younger than 15 years. There is no cure for polio, and it can only be prevented by immunization. Children across the world remain at risk of wild polio type 1 as long as the virus is not eradicated in the last remaining areas in which it is still circulating.
Despite the circulation of wild poliovirus type 1 and the variant polioviruses, incredible progress has been made. Since 1988, when the Global Polio Eradication Initiative was set up, polio cases have plummeted by 99% from an estimated annual total of 350 000.
Importation of any case must be treated as a serious concern and high-quality response efforts to reach every child with polio vaccine are critical to prevent further spread.
On 25 January 2023, the WHO Emergency Committee under the International Health Regulations concluded that the risk of international spread of poliovirus remains a public health emergency of international concern.
Women make up only 28% of the workforce in science, technology, engineering and math (STEM), and men vastly outnumber women majoring in most STEM fields in college globally. On March 2011, the Commission on the Status of Women adopted a report at its 55th session to promote women’s equal access to full employment and decent work. Two years later, on 20 December 2013, the UN General Assembly adopted a resolution in which it was noted that it is imperative for women and girls to be involved in STEM.
On the International Day of the Women and Girls in Science on 11 February 2023, Rosemary Mukui Nzunza, the head of the Expanded Programme on Immunization (EPI) at the Centre for Virus Research, the Kenya Medical Research Institute, shared her story of pursuing a career in science. She is currently in the final stages of working towards earning her PHD in Molecular Medicine.
Rosemary explains she would like girls and women to know there is enough room for everyone in science; and women should maintain healthy competition in science and go as far as they can. It also helps to look for mentors and people you can admire and follow so they inspire you to keep growing, she says.
“Research has earned this name as it means you need to go back and search over and over again,” Rosemary says. “Besides, there are no ceilings in science – girls and women can go as far as they want to.”
As a child, Rosemary Nzunza spent her free time pounding leaves, roots and tubers, using thick wooden sticks to create “medicine”. Her creativity, curiosity, and love for finding explanations for how things work made her want to teach science − or at least work in the world of science.
Rosemary never has a dull day at work. She currently serves as Senior Research Scientist and Head of Division of the Expanded Programme on Immunization (EPI) at the Centre for Virus Research at KEMRI. Her role entails monitoring quality assurance in laboratory work and biosafety and overseeing the work of the different units at KEMRI. She also represents the laboratory in key national committees in Kenya: the National Committee on Containment of Polioviruses (NTF), National Polio Certification Committee (NPCC), National Measles and Rubella Technical Advisory Committee (MTAG) and the National Polio Experts Committee (NPEC).
Rosemary joined the Kenya Medical Research Institute (KEMRI) Laboratory 23 years ago, starting her career as a research officer with the US Army Medical Research Directorate (USAMRD). In 2006, Rosemary earned her Master’s in Applied Microbiology. Back then, she was one of just two women at the unit who had postgraduate degrees under their belts. She reflects on how her male colleagues looked up to the two women as mentors, which made them feel really proud. But she notes that this also meant they were in charge of all laboratory procedures, laboratory quality, and the troubleshooting, which was quite challenging at the time.
Polio still exists
When Rosemary joined KEMRI, she was surprised to learn that the institution was tasked with supporting polio eradication. She had thought polio had been wiped out from the world a long time ago.
Presently, Rosemary and her team at the KEMRI Laboratory work meticulously on testing samples of measles, polio and rubella. They know their work is integral to saving children from the harsh effects of preventable diseases, such as polio. Their work on polio is two-pronged: they have been testing samples for acute flaccid paralysis (AFP) since 2000 and environmental surveillance (ES) since 2013. AFP is defined by the acute onset of weakness or paralysis with reduced muscle tone in children. There are many infectious and non-infectious causes of AFP. Polio, caused by wild poliovirus (the naturally circulating strain) is one cause of AFP, and so early detection of AFP is critical in containing a potential outbreak. Respiratory and stool samples are optimal for enterovirus detection. Environmental surveillance complements AFP surveillance. It entails collecting and testing wastewater samples and can help in the early detection of and response to polioviruses. By identifying polioviruses swiftly, countries can stop their spread.
At times, the 17-member team receives an overwhelming number of samples at once from countries in the Region facing polio outbreaks. This presents a challenge, as it might mean the team needs more supplies for testing and needs to work longer hours to deliver timely results.
Once they have tested samples, they interpret results for each and send them back to the country to guide further and swift action. By 3 pm Eastern African Time every Friday, the KEMRI team works to send summaries of test results on measles, polio and rubella to the national surveillance office within Kenya’s Ministry of Health and other partners. These include the WHO Regional Office for Africa (AFRO); WHO Eastern Mediterranean Regional Office (EMRO); WHO headquarters; and the US Centers for Disease Control and Prevention (CDC).
Management during COVID-19 was a challenge
One of the most difficult times Rosemary has faced in her career was the response to the COVID-19 pandemic. During that period, she felt like health workers were carrying the weight of the entire world. In Kenya, her team was tasked with supporting the government in conducting COVID-19 tests. At the time, everything seemed so uncertain. Personal protective equipment (PPE) kits looked frightening, people all over the world were dying of COVID-19, and procedures and test kits still needed validation. She remembers thinking to herself, “Someone has to do this. And it’s us, here, now.”
Agnes Chepkurui, a lab technologist, preparing samples to determine what kind of poliovirus is present in the sample. Photo credit: WHO/L. Dore
Similar to the situation health workers around the world faced, her team was also afraid of being infected with COVID-19, especially before vaccines were available. Rosemary recalls the team staying at work for long, tiring stretches, partially to avoid contact with their families, out of fear of inadvertently putting them at any risk of being infected with COVID-19. Teammates would huddle together and discuss their after-work protocol at home: slip in through the back door, disinfect clothes, clean up rigorously, take a shower, avoid all contact with loved ones, and set off on the same routine the next day before anyone woke up.
She split the team into two shifts to manage the immense workload. The aim was to prevent the team from burning out and ensuring their new work on COVID-19 didn’t slow down the other, crucial support to disease elimination that still needed to be carried out. Looking back now, Rosemary credits the support she and her team received from the management at KEMRI, colleagues, partners, friends and family with helping them stay focused and rise to the unprecedented challenges of that time.
She also attributes the success of the KEMRI EPI Division Laboratories to support from institutions across the world, including the Global Polio Eradication Initiative (GPEI) partners. She says she has always been impressed with the incredible support from WHO and the rest of the GPEI partnership, where diverse agencies come together to tackle one goal.
More mentors needed for girls to join and grow in science
The young lady who stepped foot out of her village in Machakos county – in Kenya – for the first time when she left for Eldoret to earn her Bachelor’s in Science Education has come a long way. She is keen to see other girls and women take their place at the forefront of science – but only if they have a passion for this field, she adds. Breaking into a laugh, she says there’s a lot to read and keep up with every single day. After all, science is about changing the world.
On 19 January 2023, representatives from the World Health Organization (WHO), United Nations Children’s Fund (UNICEF), and the Ministry of Health of Syria concluded a three day joint mission on polio transition planning.
The team conducted various meetings with national counterparts, United Nations agencies and other stakeholders to assess the current situation, and identify the needs and resources required to maintain polio-essential functions and strengthen routine immunization to maintain Syria’s polio-free status. As part of the mission, the team agreed on the way forward to design a roadmap to support and sustain the ongoing integration of polio assets to ensure long-term benefits for immunization and emergency response.
While Syria is a polio-free country, it is at very high risk of imported polio outbreaks. In the last decade, the country experienced two polio outbreaks, including an outbreak of wild poliovirus following an importation from Pakistan in 2013, that paralyzed 36 children. In addition, a 2017 outbreak of circulating vaccine-derived poliovirus type 2 (cVDPV2) left 74 children paralyzed. In both cases, the country managed to contain the poliovirus and stopped the outbreak in less than a year using intensive polio vaccination campaigns and surveillance.
WHO is working closely with the Government and other stakeholders to maintain highly sensitive surveillance for polio and capacities to detect and respond to polio outbreaks swiftly. Furthermore, WHO and UNICEF are supporting the country to leverage the capacity and rich legacy built from years of polio operations to strengthen the essential immunization programme and capacities to detect and respond to other disease outbreaks.
“The main goal of this mission is to ensure that the polio essential functions are well preserved,” said Dr Rana Hajjeh, Director of Programme Management at WHO’s Regional Office for the Eastern Mediterranean. “We at WHO emphasize the importance of strengthening essential programmes like the national routine immunization and also strengthening the emergency response to take advantage of all the polio assets and building health systems. Overall, Syria has integrated polio functions very well in their national immunization programme and we will do our best to continue supporting them as needed,” she added.
Polio essential functions are managed by the Ministry of Health, with the technical and logistical support of WHO. Given the importance of ensuring the sustainability of functions, with support from Gavi, the Vaccine Alliance, both partners have been able to cover critical programme needs pertaining to routine immunization, including polio.
“While protecting the success achieved in containing the poliovirus outbreaks in record time, we should combine our efforts at all levels to maintain the high levels of immunity of the Syrian people against this life-threatening disease,” said Dr Iman Shankiti, WHO Representative a.i. for Syria. “WHO is working closely with the Ministry of Health and all other partners to resume the robust immunization programme in Syria,” she added.