On 14 May 2024, the wild poliovirus outbreak in Malawi and Mozambique – which paralyzed nine children across the countries between February and August 2022 – was officially stopped. The virus, linked to a strain originally found in Pakistan, was unable to regain a foothold in the African region.
This incredible achievement was made possible by the tireless efforts of health workers and authorities across five countries – Malawi, Mozambique, Tanzania, Zambia, and Zimbabwe. Over two years, with support from the Global Polio Eradication Initiative (GPEI), they reached more than 50 million children through massive, coordinated vaccination campaigns and set up 15 new wastewater surveillance sites to quickly detect and respond to any trace of polio.
But that wasn’t all. The gender norms, roles, and relationships that can impact a health worker’s ability to access every household and guide a family’s decision to vaccinate their child were considered every step of the way. From planning campaigns to dropping the vaccine in children’s mouths, acknowledging and addressing these nuances was key to ensuring that every child was protected from this devastating disease.
For example, in Malawi, the program partnered closely with the Ministry of Gender to use a new tool first deployed during the COVID-19 pandemic – the Rapid Gender Assessment Tool. This tool analyzes the different impacts a disease has on women and men, with a particular focus on disadvantaged groups like women living in rural areas, to ensure policies and interventions around outbreaks provide equal protection for all. The insights from this tool proved vital for the wild polio outbreak in southern Africa.
The Ministry of Gender and the GPEI employed a gender-specific approach to tackle cultural barriers hindering immunization access. This strategy, informed by the Rapid Gender Assessment Tool and COVID-19 data, addressed key gaps. This included ensuring plans considered the different needs and roles of men and women in the community and tracking immunization rates by gender to identify and address any disparities in reaching boys and girls.
Gender-balanced vaccination teams navigated local customs to ensure access to all households. Community meetings at markets, schools and local health facilities further fostered dialogue with both men and women, ensuring everyone was informed and empowered to participate in vaccination campaigns.
Recognizing the importance of a data-driven approach, the country team developed additional monitoring and reporting formats to improve data collection. These formats captured information on gender not only of children vaccinated but also of polio teams working at all levels including decision-making, campaign implementation, monitoring and supervision.
Approaches like these, with gender at the center, helped the program make significant strides against the virus across southern Africa.
Malawi, Mozambique, and many countries still battle another threat – variant poliovirus – and as long as any kind of polio exists, every child remains at risk. The tools and tactics used to respond to the wild polio outbreak will be invaluable as countries work to end all forms of the virus for good.
Conflict could have the worst impact on vulnerable children, who are victims of circumstances beyond their control or capabilities. Almost a decade of conflict has led Yemen to experience devastating outbreaks of vaccine-preventable diseases, which disproportionately affect children. Key contributing factors include extremely limited public health infrastructure and services, limited water availability, and growing levels of vaccine denial and hesitancy.
“Children are particularly vulnerable to vaccine-preventable diseases such as polio, measles, pertussis and diphtheria,” said Dr Arturo Pesigan, WHO Representative and Head of Mission in Yemen. “One in 4 Yemeni children has not received all the recommended vaccinations on the national routine immunization schedule, and 17% are zero-dose children, who have not had a single dose of diphtheria-tetanus-pertussis vaccine.”
My name is Farid, and I am 35 years old. I live in the Bati Kot district of Nangarhar province. I contracted polio when I was three years old. The symptoms started with a fever, then a weakness in my left leg and weakness in my left hand. While strength eventually returned to my hand, my leg remained weak. My parents took me to the doctor. After medical examinations, the doctors said that I had polio and there is no cure. When my parents heard that I could not be treated, they took me home.
Growing up with a paralyzed leg created many challenges for me. I couldn’t play with other children but I never lost hope. I fought to live my life like other children in my community. I started attending school, then completed my studies in computer science. My parents were always supportive, especially in my studies and building my career.
In my personal life, I also encountered challenges. When I wanted to get married, I faced rejection four times from different families. They did not want to marry their daughters to me because they said I have a disability and cannot work. I’m happy my wife’s family accepted me and I now have four beautiful children. I make sure to vaccinate my children at every opportunity. I don’t want them to be affected by poliovirus like I was. I also encourage my neighbors to vaccinate their children whenever they have the opportunity.
My daily life is challenging and I face many obstacles. There are certain tasks and jobs that my relatives, friends, and neighbors can do, but I cannot. I have some land in my village where I grow things like wheat and corn to help feed my family. Because my paralysed leg prevents me from cultivating my land, I pay someone to do this for me. This often brings me disappointment.
Because I know firsthand the danger of poliovirus and how it can affect the lives of children and their families, I joined the polio eradication programme in 2017. I work as a supervisor, and my job is to train vaccination teams under my supervision. I prepare them for vaccination campaigns, make sure they receive enough vaccines and equipment, monitor their work and report their achievements at the end of each day during the campaign. On campaign days, I go out and make sure all is working well for the teams, that they have everything they need and that all children in my area receive the polio vaccine.
For those who do not want to vaccinate their children, I go to their houses and tell them that the only way to protect their children from poliovirus is by vaccinating them with two drops of polio vaccine. I also tell them that if you don’t vaccinate your children, they could be paralysed like me. I share my personal story with them and challenges that I face in daily life. In our village, we used to have many vaccine refusals, but now they are few because I take the time to talk with parents and carers and explain my situation.
Even when we are not having vaccination campaigns, I talk with people and raise awareness about poliovirus and the importance of polio vaccine. We must vaccinate our children against polio at every opportunity. Polio is a terrible, crippling disease and we cannot let any child be paralysed.
Integration involves using polio tools, staff, expertise, and other resources to deliver important health interventions alongside polio vaccines – from measles vaccines and other essential immunizations to birth registration, counselling on breastfeeding, hand soap and more. It also includes incorporating polio vaccines into other planned health interventions when possible, delivering more services with fewer resources.
There is no one-size-fits-all approach to integration. From the remaining endemic countries to countries affected by variant poliovirus outbreaks, activities must be country-driven and adapted to fit the unique challenges and needs of different communities.
Humanitarian engagement in Afghanistan:
In Afghanistan, supplementary immunization activities are essential to vaccinating children. However, in the context of an unprecedented humanitarian crisis and extremely fragile health system, integrating polio efforts with other health services has helped the program reach even more children.
Endemic transmission of WPV1 in Afghanistan has been restricted to the east region. Remaining pockets of inaccessible, unvaccinated children amid a broader humanitarian crisis pose challenges to stopping the virus for good. Today, more than two-thirds of the country’s population is in serious need of food, clean water, functioning sanitation facilities, and basic health services.
Building upon a strategy that has been in place for several years, ongoing collaboration with humanitarian organizations has demonstrated the value of integrating polio efforts with other health needs in the country. In 2023, the program began engagement with ten humanitarian partners operatingin 12 high-risk provinces for polio across Afghanistan. Through these collaborations, the program and its partners have mapped and supported communities that lack basic health services, which has helped better identify and reach children still vulnerable to polio.
Between January and October 2023, more than 1 million polio vaccinations have been delivered through the engagement with humanitarian partners. Through this effort, it’s estimated that more than 30,000 children have been vaccinated who would have otherwise remained inaccessible to the polio program during its standard campaigns¹.
The Far-Reaching Integrated Delivery partnership in Somalia:
In Somalia, children are at high risk of encountering and spreading the poliovirus due to longstanding security challenges and a lack of health infrastructure, particularly in the south-central part of the country. As a result, the country has historically low routine immunization levels and faces the world’s longest-running outbreak of type 2 variant poliovirus.
To help address these challenges, in October 2022, the GPEI partnered with the World Food Program Innovation Hub, Save the Children, Acasus, and World Vision’s CORE group, amongst others, to launch the Far-Reaching Integrated Delivery (FARID) partnership. The partnership’s primary goal is to stop poliovirus transmission and reduce deaths from preventable diseases and malnutrition.
To do this, the polio program and its partners have established a series of health camps across 20 districts in the country that provide families with vaccinations for polio and other infectious diseases, maternal health services, nutrition screening and supplements, and primary health consultations². These camps are tailored to address each community’s specific needs and aim to re-establish sustainable health systems that will continue providing primary health services on a routine basis.
Between October 2022 and June 2023, FARID partners have visited 136 high-risk communities in Somalia, reaching almost 30,000 people; vaccinating more than 8,000 children, 6,000 of which had never received any kind of vaccine; and conducting over 10,000 maternal health and 4,000 nutrition consultations³.
Read more about the polio program’s latest integration efforts here.
Islamabad – An announcement over a loudspeaker from the mosque captures the attention of parents and their children. The voice announces that a polio campaign is taking place in the settlement and vaccinators will be coming to give two drops to children under five. Eight teams of two vaccinators each are already on their way, each starting their day from the farthest house in the community and making their way to the center.
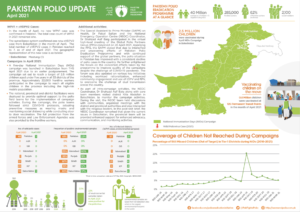
In January, when Pakistan detected a positive wild poliovirus from a sewage sample with genetic links to the virus circulating in Afghanistan, the polio teams jointly conducted a detailed epidemiological investigation to trace the routes of virus movement and identify infected populations. In a matter of weeks, a response was planned and implemented, vaccinating around 6.37 million children from 13 – 17 February. In this article we take you to an Afghan refugee settlement in Islamabad, one of the 30 districts that were covered partially and where the outbreak response focused on mobile and cross-border populations.
The story looks at three important components of a campaign: vaccinators, vaccines and tally sheets.
Vaccinators: the backbone of programme
“Who is there”, asks a man from inside the house, in Pushto.
“Polio team,” responds Salma who speaks Pushto. “We are here to give polio drops. Do you have children under five at home?”
A tall man with a three-year-old boy in his arms, opens the door and welcomes the two vaccinators. Salma introduces herself and her team member Amina and asks the father if either of their children had received polio drops that day. The father confirms that in this round, his children did not receive any polio drops.
“Can I give them the polio drops?”, asks Salma.
The father responded back energetically, “Of course, you can! I want my child to grow up healthy!”
This is when Salma opens the blue box. Inside it are ice packs and vials of oral polio vaccine. She talks to the little daughter and asks her to open her mouth and gives her two drops from the vial.
After giving the drops, she marks the girl’s little finger. “You can show this incase anyone asks if you got the polio drops.”
Amina, on the other hand, fills out the tally sheet that she will later submit to her supervisor. If this information is incorrect, it can impact the overall operational coverage data for the campaign.
On leaving the house, Amina takes out her chalk and marks the door of the house with key information that will mention what day they visited, the number of children under five in the house and if there was any child with symptoms of acute flaccid paralysis.
One house done, now on to the next one.
Vaccines: two drops for every child
“It is not always this straightforward,” says Amina. “Sometimes parents are skeptical about the vaccine and don’t want us to vaccinate their children. I often take the drops myself to show them how safe the vaccines are. When they see me taking these drops, it helps us build confidence with them.”
The polio programme has a long history of systematically listening to community concerns and addressing them, often engaging influencers such as religious leaders, to underscore the safety and efficacy of polio vaccines. This has helped address vaccine hesitancy and reached more children, building their immunity against this debilitating disease. At this settlement, occasional announcements were made through the mosque, informing people that a polio campaign was taking place and encouraging them to vaccinate their children. The result of these efforts has helped the programme significantly reduce the number of refusals across the country.
The blue box Amina carries with her has a large red “End Polio” sticker and it can carry up to 20 vaccine vials, nestled between the ice packs. Each vial contains 20 doses. She pays special attention to the box making sure the temperature is always maintained and the vaccines are kept out of direct sunlight. Vials that have been used, those that are unused and the ones in use are all kept in separate bags in the cold box.
The third important piece of a polio campaign is the tally sheet. In rudimentary terms, it is a piece of paper with many tiny boxes that deliver a telling story of number and ages of children, those who were vaccinated, those who were missed, location where the campaign is taking place and number of doses delivered. In case of any refusals, the vaccinator mentions the reason for refusal at the back of the tally sheet. It tells how well an area has been covered and the remaining gaps.
The authenticity of this data is a crucial component of operational coverage. It allows supervisors to identify gaps, present progress and advise corrective actions for vaccination teams. Each evening, this data is used to measure the campaign’s operational coverage.
In one of the houses where the vaccinators entered, the mother mentioned that the child had already been vaccinated. However, no finger of the child was marked , while the others each had a blue mark on their pinky finger. Taking no chances, the vaccinator took out the vial and gave the child drops and then marked the finger. The tally sheet cannot be marked unless a child has been vaccinated and finger-marked.
Getting past the finish line
Up until April, Pakistan has conducted four polio vaccination campaigns. With the support of 390,000 polio workers, almost 43 million children under-five were vaccinated during a five-day nationwide vaccination campaign. There are multiple campaigns planned for the year ahead, requiring hours of strategic and evidence-based planning led by the national and provincial emergency operations centres.
Leaving nothing to chance during this last 100 meter dash towards eradication, the programme has also started implementing innovative interventions, such as the nomad population mapping and vaccination of high-risk mobile populations, engaging public health students for monitoring campaigns through the Lot Quality Assurance Sampling survey and the co-design initiative that engages women polio workers to develop solutions for improving campaigns and identifying potential livelihood opportunities for them in the future.
For Amina and Salma, the conclusion of the February round meant that children under five had received the vaccine to build strong immunity against the poliovirus. However, the journey to eradication continues. After a short break, the programme will begin working on validating the next set of microplans. All of this work is essential to ensure that the virus really finds no place left to hide and no child left to paralyze.
By Rimsha Qureshi, Communications Officer, GPEI Hub Amman
Acknowledging that our common goal is to attain ‘Health for All by All’, which is a call for solidarity and action among all stakeholders;
Noting the progress achieved globally in eradicating wild poliovirus transmission since 1988, with endemic wild poliovirus transmission restricted to just two countries – Afghanistan and Pakistan;
Recalling that 2023 is the target year for interrupting all remaining poliovirus transmission globally, as per the Global Polio Eradication Initiative Strategy 2022–2026: Delivering on a Promise;
Appreciating the recent, intensified efforts made by both Afghanistan and Pakistan, resulting in a unique epidemiological window of opportunity to achieve success in 2023, as characterized by:
the geographic restriction of wild poliovirus transmission in 2022 to eastern Afghanistan and a few districts of north-western Pakistan;
the absence of any wild poliovirus case since September 2022;
the significant decline in genetic biodiversity of wild poliovirus to just a single lineage in each country; and
the successful interruption of circulating vaccine-derived polioviruses;
Emphasizing that the opportunity to interrupt wild poliovirus transmission must be seized now, given the unprecedented epidemiological progress and the inherent risks of delays in stopping polio, which would likely result in resurgence of polio;
Underscoring the ongoing risk of transmission of wild poliovirus, with detection of wild poliovirus from environmental samples in both countries since January 2023, confirming cross-border transmission ;
Highlighting that the key to success lies in reaching remaining zero-dose children (children who are un- or under-immunized) with oral polio vaccine in the most consequential geographies,1 operating within a broader humanitarian emergency response, including increasing access to all populations in some areas;
Underscoring the importance and heroic work of health workers at the forefront in insecure settings, especially women, whose support and participation is critical to the eradication effort;
Recognizing the sustained commitment by leaders at all levels, notably by political leaders and law enforcement agencies, community and religious leaders, civil society, Global Polio Eradication Initiative partners, especially Rotary International, parents, caregivers and all health workers;
Recalling that the international spread of poliovirus constitutes a Public Health Emergency of International Concern under the International Health Regulations (2005);
Appreciating the support provided by the GPEI in responding to the devastating floods affecting Pakistan and the tragic earthquake affecting Afghanistan in 2022;
Appreciating the commitment of the United Arab Emirates through the initiative of His Highness Sheikh Mohamed bin Zayed Al Nahyan, President of UAE, to promote and support polio eradication in Pakistan through the UAE Pakistan Assistance Programme;
Recognizing the longstanding support of donors like Rotary International and acknowledging the historical financial support of other Member States to the eradication effort, including the Kingdom of Saudi Arabia, Kuwait, Oman and Qatar;
Appreciating and supporting the decision of the WHO Regional Director for the Eastern Mediterranean to formally grade all polio emergencies and to apply relevant emergency standard operating procedures to WHO operations to address polio emergencies;
We, Member States of the Regional Subcommittee for Polio Eradication and Outbreaks for the Eastern Mediterranean,
DECLARE THAT:
1. We will focus all efforts on reaching remaining missed children with oral polio vaccine, within a broader humanitarian response context in the remaining most consequential geography of eastern Afghanistan and in north-western Pakistan;
COMMIT TO:
2. Mobilizing all necessary engagement and support by all political, community and civil society leaders and sectors across the Region, to fully achieve interruption of wild poliovirus transmission in the Region;
3. Facilitating the necessary support to fully implement all aspects of the Global Polio Eradication Initiative Strategy 2022–2026, including by ensuring rapid detection of and response to any poliovirus from any source, and implementing high-quality outbreak response;
4. Fostering coordination with other public health efforts, to ensure closer integration in particular with routine immunization efforts;
REQUEST THAT:
5. The international development and humanitarian communities and donors strengthen their support for full implementation of the National Emergency Action Plans to Eradicate Polio in Afghanistan and Pakistan; and
6. The Regional Director continue his strong leadership and efforts to achieve a Region free of all polioviruses for good, including by advocating for all necessary financial and technical support, reviewing progress, planning corrective actions as necessary and regularly informing Member States of the aforementioned and of any further action required through the World Health Organization Executive Board, World Health Assembly and Regional Committee for the Eastern Mediterranean.
Acknowledging that our common goal is to attain ‘Health for All by All’, which is a call for solidarity and action among all stakeholders;
Noting the progress achieved globally in eradicating poliovirus transmission since 1988;
Noting with deep concern the challenges involved in stopping ongoing outbreaks of circulating vaccine-derived poliovirus type 2 (cVDPV2) in the Region, without full access to vaccinate all vulnerable children in the affected populations;
Observing with alarm the prolonged outbreak in Yemen and the persistent restrictions on implementing outbreak response vaccination in the country’s northern governorates, and further observing that the cVDPV2 outbreak which has been continuing since 2017 is the world’s longest ongoing such outbreak;
Recognizing the Global Polio Eradication Initiative’s efforts to target its resources in the most impactful way by identifying particular areas affected by polio, including Yemen’s northern governorates and south-central Somalia, as “consequential geographies” – two of seven subnational geographies globally which together accounted for 90% of all polio cases in 2022 and which are all affected by broader humanitarian emergencies;
Recognizing the high risk of expansion of the polio outbreaks within and from the two Regional consequential geographies due to their complex emergency settings, limited access to high-risk populations, weak immunization services, gaps in coverage of supplementary vaccination campaigns, and unmitigated spread of misinformation and disinformation in northern governorates of Yemen;
Recalling that the international spread of polio is a Public Health Emergency of International Concern under the International Health Regulations (2005);
Observing with alarm that 197 children have been paralyzed by cVDPV2 in Yemen’s northern governorates, representing almost one-third of all global cases of this strain in 2022, and that the international spread of poliovirus from Yemen to Djibouti, Egypt and Somalia has been confirmed;
Recognizing the best operational approach and experience to vaccinate all children, especially infants and young children, against polio, and achieve more than 90% coverage to stop an outbreak is through house-to-house delivery of vaccination; and if that is not possible, to implement an intensified fixed site vaccination with effective mobilization of families and young children to fixed sites near their homes;
Recognizing the continued threat to all children posed by vaccine-derived poliovirus and the importance of regional solidarity and support to deliver on the goals of the 2022-2026 Polio Eradication Strategy, which have been endorsed and supported by a wide range of committed donors, such as Rotary International and Member States of the Region, in particular the UAE through the sustained commitment of His Highness Sheikh Mohamed bin Zayed Al Nahyan, President of the UAE;
We, the Member States of the Regional Subcommittee on Polio Eradication and Outbreaks for the Eastern Mediterranean:
DECLARE THAT:
The ongoing circulation of any strain of poliovirus in the Region is a Regional Public Health Emergency;
COMMIT TO:
Mobilizing all needed engagement and support by all political, community and civil society leaders and sectors at all levels to successfully end polio as a Regional Public Health Emergency;
Advocating with relevant community and subnational leaders to increase access and ensure full implementation of polio outbreak response in the most programmatically and epidemiologically impactful operational manner, ideally through house-to-house vaccination campaigns in all areas;
Focusing efforts on reaching remaining zero-dose children in the consequential geographies of the northern governorates of Yemen and south-central Somalia, working in the broader humanitarian emergency response context;
Helping to mobilize needed resources and highest-level international commitment to finalize and fully implement the Somalia Polio Eradication Action Plan 2023, in the context of competing health response priorities such as ongoing drought and the effects of the COVID-19 pandemic;
Helping to mobilize resources for the Global Polio Eradication Initiative partners to support the outbreak response in Yemen; and
Helping to strengthen coordination with other public health and humanitarian efforts in Somalia and Yemen, to ensure closer integration in particular with routine immunization and the delivery of essential health and nutrition services to children;
REQUEST THAT:
The international humanitarian and development communities scale up their support for providing essential services, including a robust vaccination response to the polio outbreaks in Somalia and Yemen using modalities that will deliver an acceptable level of coverage;
The authorities and polio eradication partners in Somalia accelerate high-quality and rigorous implementation of the Somalia Polio Eradication Action Plan 2023 to stop the longest-running outbreak in the country and prevent the further spread of cVDPV2 by the end of 2023;
10. The national authorities and the Regional Polio Eradication programme strengthen cross-border coordination across Somalia, Kenya, Ethiopia, Yemen and Djibouti, considering the documented importation of cVDPV2 from Somalia into Kenya and Ethiopia, and from Yemen into Djibouti, Egypt and Somalia, and the high risk of further instances of cVDPV2 crossing international borders;
11. Authorities in northern governorates of Yemen, all immunization partners and the humanitarian development community respond urgently to the unmitigated vaccine-related misinformation and disinformation that is being disseminated, which is risking the lives of thousands of children in Yemen and across the Region;
12. All authorities in northern governorates in Yemen facilitate the resumption of house-to-house vaccination campaigns in all areas to ensure the delivery of vaccines to the youngest and most vulnerable children, and in areas where house-to-house vaccination is not feasible, make all efforts to implement intensified fixed-site vaccination through a modality that also includes robust social mobilization and outreach to ensure high coverage; and
13. The Regional Director continue his strong leadership and efforts to support the cessation of polio outbreaks in Somalia and Yemen, including by advocating for all necessary financial and technical support, reviewing progress, implementing corrective actions as necessary, and regularly informing Member States of the aforementioned and of any eventual further action required, through the World Health Organization’s Executive Board, the World Health Assembly and the Regional Committee for the Eastern Mediterranean.
A total of nine wild poliovirus cases have been reported so far, with one in Malawi and eight in neighbouring Mozambique since the declaration of an outbreak on 17 February 2022 in Malawi. The last confirmed case to date was in August 2022 in Mozambique. The wild poliovirus in Malawi and Mozambique originated from Pakistan, one of the two last endemic countries.
Concerted emergency response launched following the outbreak in 2022 has helped increase protection among children through vaccines in Malawi, Mozambique, Zambia, Tanzania and Zimbabwe. The countries have also ramped up disease surveillance and community mobilization to help find cases and halt the virus.
“Southern Africa countries have made huge efforts to bolster polio detection, curb the spread of the virus and ensure that children live without the risk of infection and lifelong paralysis,” said Dr Matshidiso Moeti, World Health Organization (WHO) Regional Director for Africa. “We continue to support the polio control efforts across the region so that every child receives the protection they need.”
To date, 19 vaccination rounds have been concluded in the most at-risk areas and at least five more are planned for 2023 in the five countries.
Additionally, more than 10 new environmental surveillance sites have been set up over the past year in the affected countries with support from WHO. The fully operational sites are playing a critical role in the efforts to detect silent circulating poliovirus in wastewater.
“Response teams have worked intensely in the fight against polio not only in Malawi but in the rest of the neighbouring countries in a coordinated manner. We will not rest until we reach and vaccinate every child to stop polio transmission,” said Dr Emeka Agbo, acting Country Coordinator for the Global Polio Eradication Initiative in Malawi.
Reaching all households where eligible children live is critical to protect them against the risk of paralysis. The national health authorities, with support from the Global Polio Eradication Initiative, efforts are ongoing to map cross-border communities, migratory routes, border crossings and transit routes.
“Community health workers have been pivotal in the vaccination campaigns and will continue going door-to-door, bringing polio vaccines to children who might otherwise be missed,” said Dr Jamal Ahmed, WHO Polio Eradication Programme Manager.
Polio is highly infectious and affects unimmunized or under immunized children. In Malawi and Mozambique, it has paralysed children younger than 15 years. There is no cure for polio, and it can only be prevented by immunization. Children across the world remain at risk of wild polio type 1 as long as the virus is not eradicated in the last remaining areas in which it is still circulating.
Despite the circulation of wild poliovirus type 1 and the variant polioviruses, incredible progress has been made. Since 1988, when the Global Polio Eradication Initiative was set up, polio cases have plummeted by 99% from an estimated annual total of 350 000.
Importation of any case must be treated as a serious concern and high-quality response efforts to reach every child with polio vaccine are critical to prevent further spread.
On 25 January 2023, the WHO Emergency Committee under the International Health Regulations concluded that the risk of international spread of poliovirus remains a public health emergency of international concern.
The programme is focusing on reaching zero-dose children (children who are either un- or under-immunized), in identified ‘consequential geographies’.
But what exactly are consequential geographies, and why are they so vital to the global effort to eradicate polio?
In this explanatory video, long-time polio eradicator and Director for polio eradication at WHO’s Eastern Mediterranean Region, Dr Hamid Jafari, explains more.
Martha Dodray is a health worker in the Kosi River Basin area of Bihar. In order to protect all children against polio, Martha has walked, waded, boated, and rode on motorcycles to reach the communities which are spread throughout the area. The region was one of the last to have polio transmission in India, which was certified polio-free in 2014. Kosi River Basin area near Darbhanga, Bihar State, India. November 2017.
India’s journey from the world’s epicentre of a highly infectious viral disease to turning polio-free was like walking on eggshells: Every step we took mattered.
On 13 January 2023, India completes 12 polio-free years – a remarkable achievement that was made as a result of consistent, determined efforts and genuine commitment at all levels.
I spent close to six enriching years of my life serving as the project manager of the National Polio Surveillance Project (NPSP) for WHO India. My work entailed providing technical assistance and strategic guidance to the national programme. I was also in charge of poliovirus surveillance, monitoring mass vaccination campaigns, crafting corrective measures and strategies, and working closely with government counterparts at all levels to ensure every child was vaccinated enough times to build their immunity. We delivered around 1 billion doses of polio vaccine to 172 million children each year over the course of four years leading up to the last case. And many more in the years after.
Taking a step back to reflect on this journey, there were several factors contributing to the monumental success of ending polio in India. The first fundamental factor was government commitment that consistently translated into diligent administrative action at the operational level. Even the district administrators were fully aligned with and committed to taking corrective measures based on evidence: accepting programmatic gaps and challenges and then committing to addressing them urgently.
Two technical assessment missions worked on scrutinizing available evidence and analyzing the absence of polioviruses across Sudan. The first mission, conducted virtually in October 2021, shared their recommendations with Sudan’s polio eradication team to ramp up their efforts across the country.
A second official outbreak response assessment team undertook the next phase of this detailed task. They visited Khartoum and six of Sudan’s 18 states as part of their work from 24 July to 1 August 2022.
Both review teams comprised experts from the World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF). Their skills and experience ranged from global public health, epidemiology and biostatistics to surveillance, vaccine management and communication.
They worked hand in hand with the Federal Ministry of Health of Sudan, with state-level ministry staff and with health workers at ground level.
After a close review of the functionality and sensitivity of the country’s surveillance system, the assessment team noted that Sudan’s acute flaccid paralysis (AFP) surveillance indicators are indeed meeting the necessary standards. The gold standard for polio surveillance is through searching for AFP in children, and testing stool samples to confirm the presence of the virus.
All poliovirus samples collected since 18 December 2020, the date of onset of paralysis of the last child affected in the outbreak, were processed like clockwork in Sudan’s laboratory. They were reported as poliovirus negative and recorded.
The missions noted Sudan’s 14 environmental surveillance sites are also collecting and testing waste water samples regularly, in line with international protocol.
During the polio outbreak, 14 sewage samples in the country’s bustling capital, Khartoum, tested positive for cVDPV2, indicating circulation there.
As part of their work, the technical mission also reviewed the core functions of Sudan’s laboratories and the country’s preparation mechanisms for poliovirus events or outbreaks. This also included data on population immunity, childhood immunization and vaccine management protocol.
A large part of Sudan’s success can be attributed to its swift response to the outbreak as soon as it was confirmed.
The country conducted two high-quality nationwide campaigns in all 18 states to curb virus spread in November 2020 and January 2021. Each campaign delivered monovalent oral polio vaccine type 2 (mOPV2) to over 8 million under-fives.
Weighing in on this milestone, senior experts in WHO’s polio eradication programme, including
Dr Hamid Jafari, WHO Director for Polio Eradication in the Eastern Mediterranean Region, and Dr Ni’ma Saeed Abid, WHO Representative to Sudan, lauded public health officials and immunization health workers on the ground for their swift response to the outbreak.
They reiterated the importance of maintaining sensitive AFP surveillance, ensuring better outbreak preparedness and response, enhancing coverage of essential immunization, and strengthening cross-border coordination. This is crucial given Sudan remains at high risk of importation of polioviruses.
Following this extensive work, the outbreak response assessment team concluded that the spread of cVDPV2 has indeed stopped, and that the outbreak is over.
In 2021, when the news of cancer hit, Nomina Akhtar felt her world collapsing. It was discovered too late. By the time she knew, it was already stage-3 breast cancer.
Since 2015, Akhtar has been part of Pakistan’s polio programme as a community health worker. During these six years, she has found friends and well-wishers among her team members who have given her the support to carry on.
Akhtar, 43 and a mother of three continues to work for polio eradication as she undergoes treatment for cancer. “I gathered my courage and promised that I will fight till the end and live for my children. All my family, colleagues and seniors were with me whenever I needed support. That gave me courage and made me believe that I could, in fact, beat cancer.”
Based in Peshawar, Nomina’s husband and her three children, aged six, seven and 18, rely solely on her income. The lockdowns due to the pandemic caused her husband, a motorcycle mechanic, to close down his shop that has yet to reopen.
A life with cancer has been both physically and emotionally exhausting. She is undergoing both radiation and chemotherapy in Peshawar. This means a commute of almost 20 kilometers after a whole day of work.
“When I have to go for chemotherapy after work, it becomes very draining. I have to take public transport and wait at the hospital for hours. There are times when I have to return without treatment because either the machine is faulty or something else comes up. This treatment regime along with the medicine will continue for at least five years. It’s excruciatingly painful,” she says.
Polio programme: a great source of strength for Akhtar
“My colleagues are like my extended family, and I am like a sister to them. When I found out about my cancer, they wept with me. They have stood by my children and myself every step of the way.”
The supervisor of her area, Uzma Mansoor, says that when they first heard the news, they were devastated. “But it’s great to see that she has not lost hope and is fighting the disease like a champion,” she said.
The community she works in has also been incredibly supportive. “Some of the people in my work area came to know about my illness and they appreciated the fact that despite fighting cancer, I come to their doorstep during every polio campaign. Irrespective of extreme temperatures and illness, I am there to vaccinate their children and protect them from this life-threatening disease. Their support has increased manifold after this.”
Sahibullah, the Union Council Polio Officer of her area, says not only does Nomina continue to vaccinate children, but she is a role model for all other polio workers.
“It was God’s will, and we will face it with courage,” says her husband Aurangzeb Akhtar. “Despite being ill, Nomina is the one who keeps us going. She is working and earning for our family as well as motivating us to not lose hope. My children and I are so proud of her. Inshallah she will get well very soon.”
Nomina has strong conviction. She is fighting cancer and polio simultaneously, and is determined that she will defeat both very soon. “At least cancer has treatment,” she says. “Polio is incurable and the sooner we end this disease forever, the better.”
By Mohammad Shoaib, Provincial Communications Officer KP, WHO Pakistan
It’s been a long day for Dr. Nabeel Abdu Omar Ali. Since early morning, he has been going from one house to the next in a community in Aden, Yemen – listening to the concerns of parents and speaking to them about the importance of vaccination to save their children from polio. And he plans to continue till the sun goes down.
“The weather is pleasant now and I want to meet as many parents as possible, especially those who have concerns about vaccines. In a month’s time, the heat and humidity will be unbearable, making it difficult to walk from house to house,” says Dr. Nabeel.
Nicknamed “the mobile imam” by his peers, Dr. Nabeel is a pediatrician by profession, and a certified imam (Islamic teacher) from the Ministry of Endowment in Southern Yemen. He uses his religious knowledge and medical facts to educate the public about the importance of vaccination in protecting children from polio and other deadly diseases.
A few weeks back, he visited several families who were refusing vaccines in a nearby neighborhood. In addition to speaking to them about the safety and benefits of the polio vaccine, the ‘mobile Imam’ administered polio drops to his grandchildren in front of everyone at the community meeting.
“When the people saw a doctor and Imam like me vaccinating my own grandchildren, I think it was easier for them to believe that the vaccine was safe for their children too,” says Dr. Nabeel with a smile.
Reaching out to other Imams for support
Dr. Nabeel frequently reaches out to other Imams, training them about the benefits of vaccination and encourages them to share with the public during their Friday sermons.
“Imams are very influential in our communities – to raise awareness, shape social values, and promote positive attitudes, behaviours and practices. For example, a single sermon is powerful enough to change misconceptions about vaccines in some communities. If Imams are fully equipped with accurate information, it goes a long way in build trust and creating vaccine acceptance among the people – helping children in the community to stay health and free from polio and other vaccine-preventable diseases,” he adds.
The ongoing conflict in Yemen has severely damaged the health and basic infrastructure. There are frequent interruptions in power supply, and this often creates suspicion among community members as well as Imams whether vaccines are being stored safely.
“I was training a group of imams and they shared their doubts about the safety of the vaccine. They were skeptical about how refrigerators could store polio vaccines safely when there are so many power cuts in the area.”
In response, Dr. Nabeel organized a tour for the group to a vaccine storage facility where they were able to see and learn about special refrigerators that are powered by solar energy when there are power cuts.
Promoting the benefits of vaccination for over a decade
Dr. Nabeel has been working for the immunization programme in Yemen for over 12 years, partnering with UNICEF for numerous polio vaccination campaigns and routine immunization services.
When he first started out as pediatrician, he met many children who were paralyzed by polio. He felt frustrated that so many children would have to suffer for the rest of their lives by a disease that could have been easily prevented by a vaccine. That is when he decided to dedicate his time to educate caregivers and parents on the benefits of vaccination.
“There are many misconceptions about vaccines. Throughout my career I have been confronted by people who were resistant to the idea of vaccination. Some people think that the vaccine will make them infertile, while others believe it’s some kind of a conspiracy. However, my many years of work in immunization and knowledge of religious scriptures has proven to be valuable so far in building trust in vaccine in communities,” says Dr. Nabeel.
The ‘mobile Imam’ is also quite adept in working with the media to promote vaccination. He is often seen and heard on TV and radio talk shows speaking about the benefits of vaccination and answering to questions from concerned parents and caregivers.
“I use a mixed approach to address vaccine hesitancy and dispel misinformation about vaccines. Sometimes it is helpful to talk about vaccines during Friday sermon, while other times, it is more effective to explain to a caller on a radio programme why vaccines are important,” he explains with a smile.
Over four days in the middle of May, parents in the governorates of Bethlehem and Jerusalem were urged to take their children under age five to health facilities for a supplementary dose of oral polio vaccine. The aim: boost immunity to poliovirus in the face of increased regional risk.
Unlike most polio campaigns in the Eastern Mediterranean Region, the mechanism for the campaign in occupied Palestinian territory (oPt) was via health facilities, rather than house to house. This can be a major ask for parents, who must organize time and transport to get children to health facilities during a relatively brief window.
Round 1, from Monday 16 May through Thursday 19 May, tested the resolve of a community that is famously pro-vaccine (routine immunization coverage across oPt is typically between 98% and 100%), but like parents everywhere, juggling work, childcare and other commitments.
While most often, mothers took their children for vaccination, in many of the health facilities where vaccination took place, grandmothers were seen supporting mothers or even stepping into their shoes.
“I brought my granddaughters today to take the polio vaccine because their mother is studying in university and their father is working,” said Abeer Nasrallah, who brought Zeina (two) and Mariam (three) to El-Azariyeh, a Palestinian Ministry of Health clinic in Jerusalem governorate.
In Biddo, an area of Jerusalem governorate where the main UNRWA clinic serves both local families and those from more remote regions, a steady stream of clinic visitors climbed out of mini-buses and taxis after lengthy journeys.
“Many Bedouins come to us from remote areas like Bani Samuel and Beit Iksa, although the transportation from their areas is very hard for two reasons. First, the roads are very difficult, and second, there are a lot of checkpoints that could keep you waiting for hours,” said Tamam Taha, a nurse at the Biddo UNRWA health facility.
“We have good numbers of people coming to the clinic, both refugee and non-refugees, and we give the vaccine to all of them,” she said.
One of the groups she served was headed by Samar Al-Sheikh, a mother of one who arrived with three girls in tow.
“I brought my brother’s daughters because he can’t come. Usually, I would walk from my home, but I took public transportation today because I have three kids with me. It was hard to manage them, but it’s important to give them the vaccine,” she said.
In some cases, the hurdles parents faced to bring their children to health facilities were starkly visible.
Nidal Kandeel, father of Janette (three) and Jolan (21 months), arrived at Biddo UNRWA health facility on crutches.
“I got an injury in my work a year ago, and I’m now disabled for the rest of my life. It was hard for me to come to the clinic using public transportation, but I know how important it is for my children to take the polio vaccine, and this is why I am here,” he said.
While the results of this preventative campaign are still pending, clinics promoted the campaign heavily through their own social media groups, and health workers explained that logistics aside, it wasn’t difficult to convince Palestinian parents of the need to vaccinate under-fives.
“There is a lot of demand for this vaccine. Many people have been coming since this morning to get their children to take the vaccine. In the last hour, we have vaccinated more than 100 children,” said Khawla Abu Khdeir a nurse running the registration desk at El-Azariyeh.
Following the four-day vaccination blitz at health facilities, nursing teams will review registers of children vaccinated and cross-reference these with patient lists. Parents of children who weren’t vaccinated will be telephoned and efforts made to reach those children through in-clinic follow-up or outreach.
Round two of the bivalent oral polio vaccine (bOPV) campaign is expected in mid to late June, with the aim of raising immunity levels in these two governorates.
Palestine has been polio-free for more than 25 years, thanks to a robust routine immunization programme and a strong culture of vaccine acceptance.
But following the detection of circulating vaccine-derived poliovirus type 3 (cVDPV3) in sewage outflow in Wadi Alnar site, a junction between wastewater coming from inside the green line with wastewater coming from Bethlehem and Jerusalem, the Palestinian Ministry of Health launched efforts to boost immunity in the areas deemed most at risk.
The campaign was carried out with support from WHO, UNICEF and UNRWA’s Palestine country offices.
WHO’s Palestine office provided technical support to the Ministry in planning and executing this campaign, drawing on the extensive expertise of our regional polio eradication programme.
The vaccination campaign in Palestine is part of the global effort to eradicate poliovirus, spearheaded by the Global Polio Eradication Initiative.
It is a hot afternoon in Chagai, a small community on the south bank of the River Gambia when the polio vaccination team arrives to a rapturous welcome. Children and women jump to their feet, some waving and swinging their hands as they pound their feet on the ground in near perfect sync with the beat of the drum.
This excitement is caused by one certain member of the vaccination team wearing a bush hat and playing the drums. Lamin Keita, 60, is a cultural musician supporting the vaccination team in raising awareness about polio and encouraging parents to vaccinate their children. Lamin, popularly called Takatiti, because of one of his songs, is immediately surrounded by excited children, as he adjusts his beats to respond to the ecstasy and rigor of the dancers.
“When I arrive on the back of a pick-up truck with my megaphone and drums, children from the communities run after us in full excitement and jump up and down and ask me to play my drums,” Takatiti explains.
This is what Takatiti is popular for – pulling crowds with his drums to communicate important messages like polio vaccination. For almost four decades, he has toured communities in the region, accompanying health workers as they seek to persuade parents and caregivers to vaccinate their children during mass vaccination campaigns like the polio campaign.
Local voices are the most powerful voices
Building trust in vaccines among parents and caregivers is the first critical step towards achieving high immunization coverage to stop the spread of polio. UNICEF, as a leading partner of the Global Polio Eradication Initiative (GPEI) for social and behaviour change, supports the government in strengthening engagements with communities, as the voices of local leaders and influencers like Takatiti play a powerful role in helping allay fears and concerns of parents and caregivers about vaccines.
“I have been making town announcements since the mid-1980s. I am aware of polio and its terrible consequences. Families hear myths and rumours and get concerned about vaccines. As they already know and trust me, I try my best to give them accurate information and clear their doubts, so that they can vaccinate their children against polio and other dangerous diseases,” Takatiti says.
“It’s important to deliver messages that are supported by facts in an effective way”
Days before the start of a polio vaccination campaign and during the campaign itself, Takatiti walks up and down the streets of villages, playing his drums and using his megaphone to talk to communities about the dangers of polio, how vaccination is the only way to protect children, and that polio vaccines are safe and free.
“I always try to promote peace and healthy life for all. It’s important to deliver messages that are supported by facts in an effective way. The Government and UNICEF provided me correct information and facts about polio and vaccines, so I am happy to volunteer for the campaign.”
A country mobilizes to stop polio
“If people trust health workers to cure other diseases, then it makes sense to trust the same health workers to protect our children from polio. Health workers even give the polio vaccine to their own children – so we should not doubt their good intentions. It is my job to let people know this truth, without offending them, and encourage them to vaccinate their kids,” Takatiti said.
In August 2021, The Gambia declared a national public health emergency in response to outbreaks of non-wild variants of polio in the country.
The Gambian government, with support from WHO, UNICEF, US Centres for Disease Control and Prevention (CDC)and GPEI partners, quickly responded and started preparing for nationwide immunization campaigns – managing supply and safe storage of vaccines, strengthening surveillance and monitoring, training health workers and vaccinators, and engaging with local leaders and influencers to build trust in vaccines.
The country undertook its first national polio vaccination campaign in November 2021 and followed up with a second round in March 2022.
Thanks to thousands of health workers, vaccinators, and community influencers like Takatiti, the vaccination campaigns have reached over 380,000 children aged five years and below in The Gambia.
Infectious diseases like poliomyelitis (polio) know no borders. Importation and subsequent spread of the virus led to the paralysis of 34 children, and 26 others tested positive without developing symptoms of paralysis. Extensive immunization efforts began in February 2021, and no child, adult or environmental sample in Tajikistan has tested positive since August 2021.
The outbreak in Tajikistan marked the first detection of circulating vaccine-derived poliovirus type 2 (cVDPV2) in the WHO European Region. It is now the first cVDPV2 outbreak in the world to be declared officially closed following supplemental immunization using the novel oral polio vaccine type 2 (nOPV2).
The Region has been free of endemic poliovirus since 2002. Detection of just 1 case of polio – whether from a wild or vaccine-derived poliovirus – is considered an outbreak, and requires an immediate and comprehensive response.
“Tajikistan’s success in stopping this outbreak is a major achievement and a clear demonstration of the highest level of political commitment of the Government of Tajikistan,” says Dr Hans Henri P. Kluge, WHO Regional Director for Europe.
“This outbreak and the subsequent response came at a time when the health system was already overstretched by the COVID-19 pandemic and the country was mounting a massive COVID-19 vaccination drive. Both outbreak responses had to be done without disrupting the vitally important provision of other routine vaccines to children. We acknowledge the efforts of the Ministry of Health over the past several years, which resulted in a resilient immunization system able to successfully manage all these competing immunization priorities.”
Actions taken to stop the outbreak
Following confirmation of the outbreak, the Ministry of Health and Social Protection of the Population took immediate steps, with support and guidance from WHO and other Global Polio Eradication Initiative partners. Actions included enhanced poliovirus surveillance, intensive contact tracing and a thorough review of immunization coverage at subnational levels. A rigorous risk assessment was conducted to determine the outbreak response scale and choice of vaccine, and the country rapidly completed a comprehensive verification process for readiness to use the nOPV2 vaccine.
In February 2021, a high-quality nationwide inactivated polio vaccine campaign was conducted to close the immunity gap against poliovirus type 2 among the more than half a million children born from 2016 to 2018 who had been left vulnerable as a result of global inactivated polio vaccine (IPV) supply constraints following cessation of trivalent oral polio vaccine use.
From June to September 2021, 2 nationwide and 1 subnational nOPV2 immunization rounds were implemented for all children under 6 years of age, with coverage confirmed (through external assessment) to be greater than 95%. Extensive social mobilization and communication strategies were deployed to reach groups who were at risk of being missed, including internal migrants in urban areas and unregistered children.
Assessment of the outbreak response
Several criteria must be met to officially close an outbreak, including at least 6 consecutive months in which no poliovirus is detected. The independent experts of the Global Polio Eradication Initiative who conducted the assessment in Tajikistan also looked at the performance of routine polio vaccination, the coverage achieved during the supplemental immunization rounds, and the capacity and sensitivity of the polio surveillance system to detect any poliovirus circulation.
Following the thorough assessment, which included briefings at the national level and field visits to national referral hospitals, public hospitals, polyclinics, regional and district immunization programme offices, and public health centres, the team recommended closure of the outbreak.
nOPV2 – a new chapter in global efforts to eradicate polio
Ending this outbreak using nOPV2 is an important milestone for the global polio programme. The innovative vaccine is a key part of the new strategy to stop cVDPV2s. Clinical trials show that nOPV2 is safe and effective, and more genetically stable than the traditional type 2 oral polio vaccine.
Since the rollout of nOPV2 began in March 2021, over 265 million doses have been administered across 14 countries. The majority of countries using the vaccine have also managed to stop transmission of cVDPV2; however, this is the first official closure of an outbreak to take place following nOPV2 use.
In addition to successfully halting transmission and lowering the risk of infection for millions of people, Tajikistan contributed to global research on nOPV2 with the support of WHO through an nOPV2 immunogenicity study. The country also participated in a global vaccine wastage study.
Dr Pascal Mkanda, Director for the Polio Eradication Programme in the World Health Organization’s Regional Office for Africa (AFRO), also famously known as our ‘villager in polio’, is this month (February 2022) entering a well-deserved retirement. Pascal’s contribution over the years to polio eradication in Africa, and indeed broader immunization, is second to none.
Under Pascal’s stewardship and leadership, wild polioviruses were successfully eradicated from the continent, the polio infrastructure integrated into broader public health efforts, new technologies and innovations for reaching the most marginalized children established and new vaccines successfully rolled-out. His expertise, knowledge, dedication, zeal, and passion to work and more importantly his mentorship to fellow colleagues and health workers to alleviate the lives of vulnerable children across the continent, will be sorely missed.
“I have worked with Pascal for close to 7 years, and during that time, I have witnessed first-hand Pascal’s dedication, and what he often refers to as ‘tough’ decision making, which we owe to the successes we have seen in the polio program” said Dr Matshidiso Moeti, WHO Regional Director for Africa.” My first interaction with Pascal was during the first meeting for Program Managers in the region, in Johannesburg, South Africa, in 2016. During this meeting Pascal expressed very passionately that the only way we can get results in Polio is by holding everyone accountable. To use his words, global health, very much like soccer, requires a coach to put his best players on the field. Throughout the continent, children are healthier and better protected from infectious diseases, most notably of course from polio, thanks to the tremendous efforts and tireless work of Pascal. This continent owes a huge debt of gratitude to Dr. Mkanda. On behalf of all mothers of Africa, I can simply only say one thing: Thank you, Pascal!”
“Rotary and Rotary members across Africa have been at the forefront in the fight against polio since President Nelson Mandela shouted his rallying call in 1996 to ‘Kick Polio Out of Africa’,” according to Dr Tunji Funsho, Chair of Rotary’s Nigeria National PolioPlus Committee and one of TIME Magazine’s 100 Most Influential People in 2020. “We went from 75,000 children paralyzed each year, all over Africa in 1996, to Zero wild polio cases since 2016. An unparalleled public health achievement, which could not have happened without Pascal’s leadership, engagement, and expertise. On behalf of Rotary members across Africa, Pascal – thank you so much for everything that you have done. We all wish you a more than well-deserved retirement.”
“I can only echo what others have already said,” commented Professor Rose Leke, Chair of the African Regional Certification Commission, which independently certified Africa as wild poliovirus free in 2020. “It was my great honour, and together with my fellow Commission Members, to certify our continent free of all wild polioviruses. Dr Mkanda and his team across the continent were absolutely instrumental in this. As Director of Polio in the Region, he exhibited great leadership. He and his team helped us verify the absence of wild poliovirus, even from the most inaccessible and remote areas of Africa. They helped ensure that children everywhere, no matter where they lived, were reached with the life-saving polio vaccine. Dr Mkanda demonstrated truly the best of Africa. All I can say is a tremendous ‘thank you’ to him and his team. I wish him well in all his future endeavours.”
Dr Mkanda’s career started from humble beginnings in a small and remote village, Chintheche in northern Malawi, with virtually no infrastructure. Pascal, son of a stay-home mother and a primary school teacher in Nkhata Bay, started making ‘tough decisions’ very early in life. At a tender age of 13, he and his elder brother Justin left their home on foot, and walked 18 miles with no shoes, to look for what would eventually be their family’s home in search of a better education for him and his siblings.
This was only the beginning of the ‘tough decision making’ that Dr Mkanda is well-known for today. The young Pascal Mkanda continued with his education and was eventually identified as his district’s best performing student. At the time, the president of Malawi, His excellency Dr Hastings Kamuzu Banda, had initiated a programme offering the brightest pupils (top 2.5%) from each district in Malawi irrespective of sex or socio-economic status, the opportunity to attend higher education, at the prestigious Kamuzu Academy, and through this educational opportunity, Dr Mkanda performed exceptionally and was awarded a full sponsorship to study Medicine in the United Kingdom where he attained a medical degree at the Imperial University College London.
To just show how intelligent he was – Pascal was afforded an opportunity to also study for a degree in microbiology/infectious diseases at the London School of Hygiene and Tropical Medicine while at the same time pursuing a degree in medicine. In later life he went to the Rollins School of Public Health at Emory University in Atlanta, USA, and obtained a Master of Public Health.
Putting his theoretical knowledge into practical experience, it was not long before Dr Mkanda began making a very real impact on Malawi’s public health system, improving the health and lives of remote communities. He rapidly developed a reputation for solid, practical and effective work. Here he developed the traits that would characterize his entire career and for which he became so respected: the courage of standing up for his convictions; an ability to identify and promote new and excellent talent, that would help him establish relevant and pragmatic support teams across the region; a fearless dedication to step out of group thinking even if it meant standing alone against adversity; and, an absolute and unwavering commitment to achieving results.
Respected by peers and more importantly communities themselves, he rapidly caught the attention of the international development community while working in some of the most remote communities in Malawi. During a visit by the USAID Mission in Malawi to Nsanje District Hospital in the south of Malawi, Dr Mkanda’s work caught the attention of the Country Representative who immediately recommended him for a USAID-sponsored Global Health Programme which subsequently led to the beginning of his international career.
Starting out as a National Programme Officer in Malawi for the World Health Organization, and moving on to Zambia as an international staff, he met and established a long-term friendship with Dr Francis Kasolo (former VPD Regional Virologist). By the year 2000, Dr Mkanda was managing immunization activities for Eastern and Central Africa and would eventually lead polio activities in Nigeria and Ethiopia.
It was during his time as WHO Polio team leader in Nigeria and Ethiopia that these countries were able to make significant inroads in interrupting wild polio transmission. One contributing factor for this achievement was the introduction of the famous accountability framework that held every staff accountable for their work with those underperforming being replaced by “fresh legs on the football field”, in Pascal’s own words.
It was therefore not a surprise that when the position of WHO African regional polio coordinator was advertised, that Dr Moeti – then the new Regional Director for Africa – appointed Pascal to lead the fight against this disease in the Region.
Never losing focus on the need to reach every last child with polio vaccines, with support from Dr Moeti and the Bill and Melinda Gates Foundation, Dr Mkanda established a regional center for the Geographic and Information Systems (GIS). According to Dr Joseph Cabore, Director of Programme Management at WHO’s African Regional Office: “One very critical contribution by Pascal to the regional office, is the introduction of innovative technologies and solutions. It’s amazing to see in real time, where our frontline workers can reach during mass campaigns and outreach activities. Pascal, thank you for ensuring that we remain accountable to our African children and their families.”
“It has been a privilege to work alongside Dr. Mkanda in pursuit of a polio-free world,” said Dr. Chris Elias, President of Global Development, the Bill & Melinda Gates Foundation. “His commitment and dedication to eradicating polio have been vital to helping protect millions of children from this debilitating disease and helped achieve a WHO African Region that is now free of wild polio – a monumental achievement in global health. I am forever grateful to Dr. Mkanda for his work and partnership on ending polio.”
Michael Galway, Deputy Director Polio at the Bill & Melinda Gates Foundation, added this personal comment: “Working with Pascal over the past decade has been one of best parts of the job in helping to get rid of polio in Africa. I’ve always appreciated the passion and conviction he’s brought to the work, and his keen understanding of how to get the polio programme to perform at its best in some of the most difficult places. He’s been a role-model and a friend, and I’m grateful for both!”
It was in Nigeria – for a long time the global epicentre for polio – that Pascal’s leadership really came into its own.
Dr Faisal Shuaib, Executive Director of the National Primary Healthcare Development Agency in Nigeria, said: “Pascal Mkanda’s contribution to making Nigeria free of wild poliovirus cannot be overstated. It took innovative strategies and approaches to ensure that every child could be reached, and virus transmission effectively tracked, in hard-to-reach and inaccessible areas. Pascal helped develop and trailblaze novel approaches which ultimately led to our success. It really took rewriting the strategic rulebook, and these approaches are now being implemented in other high-risk polio areas. All for the benefit of the most marginalized children. Thank you, Pascal, we could not have done it without you and your leadership. We will miss you!”
Indeed, it is this same leadership by Dr Mkanda that led to the establishment of the Rapid Response Team (RRT), coordinated by Dr Ndoutabe Modjirom in the WHO Regional Office in Brazzaville to tackle the remaining form of polio, the circulating vaccine-derived polioviruses (cVDPVs): “Pascal, you are leaving big shoes to fill. We will need your kind of leadership to end all remaining forms of polio in our region once and for all. It will not be easy to finish this job without you.”
Pascal will be missed, as underscored by Aidan O’Leary, Director for the Global Polio Eradication at WHO Geneva. “On behalf of all partners and stakeholders, the Global Polio Eradication Initiative wishes you all the very best in your retirement and/or in your next chapter of life. We know of course that you will stay engaged in one capacity or another in this fight, and we look forwards to one day, very soon, to celebrate together with you the victory over all forms/types of polio worldwide once and for all. A big thank you, in particular for your leadership in certifying the Region free of wild polioviruses and for facilitating the introduction and roll-out of novel oral polio vaccine type 2.”
Congratulations on your retirement! Now you’ll have more time for sleeping in, fishing, reading, golfing and if you want to be a DJ-from G22, where it all started!
Dr Nida Ali joined the Polio Eradication Programme in her native Pakistan in 2017. A graduate of the medical faculty at Hamdard University in Karachi, she reflects on her time with the programme, the role of women and the eradication of polio in one of the last countries where it remains endemic.
I worked for the polio programme in Pakistan for four years and 10 months. It wasn’t easy – but then, what is? I look back at those long years and cry at the times when I laughed and laugh at the times when I cried. The programme gave me lot: exposure, experience, learning opportunities, knowledge, skills, and excellent colleagues from whom I learned a lot. But the ultimate gain was, of course, the children in my own country, including my son, who took polio drops in every polio immunization campaign.
I joined the programme in 2017, as Polio Emergency Response Officer in the provincial office in Punjab. I’m originally from Rawalpindi and before joining the programme, I worked on a government-led Reproductive Health programme which sparked my interest in public health.
I’d read about polio as part of my paediatrics study at medical school but I didn’t see a case of polio until I joined the programme. It was WPV (Wild Poliovirus Type 1) and it was in Punjab, a very small child who wasn’t even a year old. The second case I saw was a case I investigated when I was working as a Polio Eradication Officer in Islamabad. All the signs were there – the child lived in a very densely populated household where the hygiene conditions weren’t good, in a part of town where a lot of travellers were coming and going. He’d also been what we call a ‘refusal’, meaning that his caregivers had refused to allow him to be vaccinated. I examined the child and it was a classic case of Acute Flaccid Paralysis, or AFP, one of the signs that the virus may be circulating in the community. The ankle reflex was present but the knee reflex was lost. We sent samples to the laboratory and it was declared as a positive case of polio.
I held a number of roles during my time with the programme – Area Coordinator, Rapid Response Officer, Divisional Surveillance Officer – and I was fortunate enough to travel to other provinces. I went to northern KP (Khyber Pakhtunkhwa) to respond to a WPV outbreak, and to southern KP and Gilgit-Baltistan for post campaign monitoring. I learned some phrases of the local language in northern KP – how many children do you have in the house, the numbers from one to ten, how many children are vaccinated, can I see their finger mark – phrases that helped me make a connection with mothers and understand their responses. I also used to take out my phone and show them photos of my son – he was four years old at the time – and tell them that he takes the polio drops in every campaign. It was great to make such a human connection and I was able to convince many refusals that way.
Seeing the programme at field level gave me great insights but so did working at the National Emergency Operations Centre (EOC) in Islamabad. It’s where all the work and knowledge comes together, and where staff from all the different the provinces come so it was a great opportunity to meet them and exchange experiences.
Women make up around 40 percent of the polio programme but mainly as frontline workers who go from house to house to vaccinate millions of children across the country. There aren’t so many women at higher levels, often because women don’t apply for these positions, which is a shame. On many occasions I found myself to be the only woman in a large meeting room, particularly the meetings where policies and protocols are discussed. I think the presence of more women in leadership roles will bring an interesting perspective to the programme, particularly given our roles as mothers and caregivers.
Today I’m in Atlanta, studying Global Health at Emory University. It was my experience with the polio programme that helped me get through all the stages of obtaining scholarship and a placement in such a reputed University. This is an interesting opportunity of learning from the experts, which again, is not new to me as this is exactly what I’ve been doing at the polio programme in Pakistan. I’m not sure where this will lead me – back to polio or to another part of public health, I don’t yet know. All I know is that I will go where my expertise leads me.
I hope one day I can tell my son the story of how polio was eradicated and how no child will ever be paralyzed by this virus again. I hope by that time, we direct our resources for protecting children from other diseases or, even better, to curb the infections that have potential to lock the whole world down.
A poliomyelitis (polio) vaccination campaign for children aged 6 months to 6 years who missed routine polio doses in the past will begin in Ukraine on 1 February 2022. This catch-up campaign is part of a comprehensive response to stop an outbreak of poliovirus first detected in Ukraine in October 2021. This first stage will last 3 weeks and is expected to reach nearly 140 000 children throughout the country.
Years of low immunization coverage in Ukraine have created a large pool of unvaccinated or under-vaccinated children who are vulnerable to polio. While routine immunization coverage has gradually increased over the past 6 years, in 2020, only 84% of 1-year-olds received the required 3 scheduled doses of polio vaccines by 12 months of age.
The immediate goal of the campaign is to reach the WHO-recommended level of 95% vaccination coverage of eligible children.
Background
The polio outbreak in Ukraine was confirmed on 6 October 2021. Poliovirus (circulating vaccine-derived poliovirus type 2) was first isolated in a 17-month-old girl in the province of Rivne who developed acute flaccid paralysis. Analysis of all her contacts found that 7 household contacts (siblings) and 8 community contacts in Rivne as well as 4 cousins in the province of Zakarpattya (who had had contact with the girl’s siblings) also tested positive, but did not develop paralytic symptoms.
A second case with acute flaccid paralysis (a 2-year-old boy in the region of Zakarpattya) also tested positive for poliovirus, with onset of paralysis in December 2021.
The isolated strain of the virus found in both paralytic cases and their contacts is linked to a poliovirus in Pakistan, which was also the cause of several cases in Tajikistan in 2020–2021.
Comprehensive plan to stop the spread of poliovirus
Following an initial local vaccination campaign, conducted where the first case was detected, a comprehensive polio outbreak response plan was approved by the Ministry of Health in December 2021.
The first stage of the plan will provide inactivated polio vaccine (IPV) to children aged 6 months to 6 years who have not received the required number of doses. In the second stage, all children under the age of 6 will be vaccinated with oral polio vaccine (OPV), even if they have received all their scheduled vaccination doses. This is necessary to protect children from infection and to stop the circulation of the virus. Dates for the second stage are pending.
Contracting the infectious virus at 11 months of age, few believed Soni would ever be able to work. Today, she’s a nominee for one of Pakistan’s most prestigious awards.
Soni started out in the programme in 1999, initially as a vaccinator. Now a mother of three children, these days, Soni works with the programme as a social mobilizer. Her role includes dispelling people’s misconceptions about the vaccine and engaging with parents about the importance of vaccinating their children.
When Soni received a notification from the Government of Pakistan that she had been selected for a Presidential Pride of Performance award, which honours individuals who are extraordinary in their field of work, she didn’t quite know how she felt. “I’m not really interested in accolades, but my son and my husband were very excited” she said.
Soni says her work with the polio eradication programme has given her life meaning and purpose. “People would look at my leg and say, ‘How will she work?! She can’t work. But when I started working, then everyone could see, ‘yes, yes she can’,” she says.
“The polio programme has given me so much confidence. After I started working in polio, I had the confidence of meeting new people. Meeting family, going to weddings, all of it became easier. Before that, I had no confidence to even step out of the house,” she continues.
Soni recalls how hesitant her father was when she first told him she wanted to join the programme. “He was concerned I won’t be able to manage because of my health, but he understood very soon that this was something I just had to do. He told my mother ‘let her do it’.”
During her early training as a vaccinator, Soni recalls the words of one of her trainers – ‘If you can save one child from polio, then you would have served the purpose of your life’. “I knew, then, this was it, “she says. “This is what I had to do.”
The year Soni was diagnosed with polio – 1984 – nearly 200 other children in her neighbourhood of Liaquatabad in Karachi were also diagnosed with the virus. At the time, there were no door-to-door campaigns and children could only be vaccinated at health centres.
Today, Pakistan and Afghanistan are the last two countries in the world where wild poliovirus is endemic. In 2021, only one child was paralyzed by the virus in Pakistan and four in neighbouring Afghanistan. In 2020, a total of 84 cases were reported in Pakistan and 56 in Afghanistan.
The eldest of six siblings, Soni came from a very conservative family, where her grandmother would not let children leave the house. “In our family, all the children were born at home because the women were not allowed to leave the house, and so I was never taken to a health centre for vaccination.”
“My father always lived with the regret of not vaccinating his daughter,” she says. “Often parents make these decisions, and it is the child who has to suffer for all their life.”
Both Soni’s parents tried everything they could to heal her condition – visiting different doctors, acupuncture specialists, and anyone they could find who might offer any assurances. She also went through a very extensive operation, with steel bolts put in her leg resulting in excruciating pain that lasted for months.
“No matter what you do, whatever you try, there is no cure for polio,” she says. “I wanted to study sciences, and my teacher didn’t allow me to because she would say how will you stand in labs all day. I would go to college and one of the women in the bus would see me and say ‘Look at her, such a beautiful girl and look at what happened to her foot’.”
Soni says that when she is working on campaigns and some people see her, they immediately want to vaccinate their children, while others question why she is telling them to vaccinate while having polio herself.
“To them I say, I am here because I know exactly how hard it is if you are not vaccinated.”
Anand Kumar learned to walk later than other children. When he did, he walked with difficulty, dragging his right leg. He was around three years old when his parents reached out for a diagnosis. “I’m sure that they tried all the doctors in Bangalore to just get it corrected. But the thing was: couldn’t do it,” he says.
His route to being an athlete was not remotely expected when he was a toddler. The doctors’ verdict ruled out recovery. Kumar had suffered irreversible damage to both his right arm and right leg as a result of an infection with poliovirus during infancy. He was unlucky: in most babies, the disease would have passed all-but-unnoticed, mistakable for a bout of the flu. But approximately one in 200 poliomyelitis patients suffer permanent paralysis. Around 5 – 10% of people paralysed risk dying if the muscles in their respiratory systems are immobilised.
Although the world’s first safe and effective polio vaccine – the Oral Polio Vaccine (OPV)1 – had been introduced decades before, and countries like the USA were newly polio-free, in the early 1980s, just 2% of India’s children had been administered the recommended three doses. During 1981 alone, India recorded more than 38,000 polio cases. The real tally may have stood much higher: researchers have pegged the actual incidence during the 1980s at closer to 200,000 cases a year.
By 1990, the annual infection figures were in decline. But the trend towards zero cases was halting, and jagged. In 2002, India’s depleted but persistent polio case-load jumped six-fold. A year later, India was home to 83% of all the new polio cases in the world. Uttar Pradesh alone, the vast and troubled northern state in which UNICEF had recently been obliged to launch a social mobilisation scheme to counter vaccine hesitancy, accounted for 64% of the world’s polio burden. The Global Polio Eradication Initiative redoubled its immunisation efforts, but as certain leading anti-polio campaigners would later admit, to some onlookers, the challenges of elimination in India looked at times simply too steep to surmount.
Meanwhile, in the late 1990s, Anand Kumar was leaving school for college with the frustrated awareness that he had been passed over. “Due to my disability, I was not active like other kids, so I was not taken into consideration for cultural activities or sports,” he says. “I was feeling that I was missing something.”
As such, he found his way to badminton late: aged nineteen, years too old to be taken on as a beginner by the coaches he approached for training, but newly cognisant of the existence and possibilities of para-sport. He watched the coach at his local club from the bleachers – “luckily, the coach was a left-hander, and I’m always a left-hand player” – then practised the technique he observed on the court on his own. He improved quickly, began beating his able-bodied opponents.
In 2001, he was invited to represent India at a para-badminton tournament in Germany. “I thought, okay: I’m defeating the able-bodied players – and I can defeat the disabled players also.” Instead, he lost every match. Looking back, he calls it “a very good experience.” That was the year he decided to practice “most seriously.”
Success, Anand Kumar earnestly points out, has not come easily. “I have had to prove myself in each and every field,” he says. He meets young players inspired by his achievements – some 110 medals, including an Asian Games bronze, a BWF Para-Badminton World Championship doubles gold and a prestigious Ekalavya sporting award – “but I always like to share my other part of the story – which was very difficult, in which I struggled hard to come to this level,” he says. “Like, I started in the year 2001 to play an international tournament, but it took 15 long years to be a World Champion”.
That struggle has only been incidentally shaped by his disability, he clarifies. “Life is always challenging, whether it’s in an able body or a disabled body,” he says. The message he shares with the students he now coaches at his own Academy, able-bodied and disabled alike, is to take up life’s challenge with determination – put simply, to never give up.
Likewise, it took a number of tacks and switches to drive down polio in India – the introduction of improved bivalent polio vaccine in 2010; the institution of rolling vaccination at strategic transport hubs; hand-washing and sanitation campaigns to tackle the diarrhoea epidemic that was found to be weakening polio vaccine effectiveness, to name just a few – but in 2012, India finally arrived at zero polio cases.
“Today we are calling India polio-free,” Kumar says. “It’s only because of vaccination.” He’s right. But he’ll also tell you that no victory is ever quite that straightforward.
Health interventions and immunization activities are most effective when delivered by women. During each nationwide polio vaccination campaign in Pakistan, women make up around 62 percent of the 280, 000+ frontline workforce vaccinating millions of children across the country.
With each campaign depending on the dedication of staff to reach all children, given their trusted roles and responsibilities in communities, female polio frontline workers are playing a key role in eradicating polio.
Breaking barriers to immunization
After three years as a monitor of campaign activities, Zubaida Bibi has progressed from being a polio team member to a team leader in Khyber Pakhtunkhwa province in the country’s north, one of the most affected areas in Pakistan.
Breaking the gender-related barriers to immunization, Zubaida travels extensively including hard-to-reach areas. Not even the winter season, when the roads and tracks are covered with snow, deters Zubaida.
“It leaves us with no option but to travel for miles and hours on foot to reach the children,” she says “Despite the challenges, I always try and motivate my teams, telling them that we are on a national mission to save the future of our children,” she says.
“It gives me a feeling of gratitude and satisfaction when the community appreciates our efforts for improving the health of their children,” adds Zubaida.
Building trust
For nine years, Shumaila Majeed has worked as a community-based health worker in Lahore, with a firm belief in empowering women and supporting their important presence in the polio programme.
Mothers would frequently ask her about the safety of the polio vaccine. “I would always tell them that the polio vaccine is totally safe for their children and build their trust,” says Shumaila.
“It’s very important to have women in every walk of life,” she explains. “Not only because women and grandmothers feel more comfortable when their children are vaccinated but to give more opportunities for woman to grow and excel.”
Through her work Shumaila wants to give young girls a message: stay focused on their goals and leave no stone unturned to make their dreams come true.
Persuading parents
In Pakistan, a significant number of parents and caregivers still doubt the effectiveness of vaccines. Karachi has long been a core reservoir for the poliovirus, with continuous and intense circulation.
Shagufta Naz, a community-based health worker in charge of Gulshan town, has been working for 21 years to ensure all children in her area are vaccinated on time. “Initially, parents used to hide their children from us due to their fear,” she explains.
Everyone who works with Shagufta is immediately impressed by her great care, her attention to detail and her meticulous record-keeping which is key to achieving vaccination targets. As a result of Shagufta’s hard work, vaccine refusals have reduced significantly. Her work is now so highly regarded that some parents will only have their children vaccinated by Shagufta, asking for her by name with each polio campaign.
“I got to know the community very well, built their trust,” she explains. “I know every pregnant woman and can tell you when she is due. Now, mothers regularly ask me about the next vaccination campaign.”
Going against all odds
Gul Parana, a Tehsil Communication Officer for the polio eradication programme in Balochistan province in the country’s southwest, recently graduated with a master’s degree.
Assigned to raise awareness about the benefits of vaccination in Chaman District, one of the most challenging areas for the polio programme, she is proud of her work despite many challenges.
“Since Chaman is a very remote and conservative area, it’s not easy for a young girl like me to go out of the house. Most of my friends are not allowed to work. But I have a mission to save our children and give them a healthy future,” she says.
With support of her family, Gul Parana has become a symbol of strength for the girls of her locality. “I want to inspire other girls so they can also get an education and work. We need to have equal opportunities for every girl in Balochistan,” she adds.
In April:
No case of WPV1 was confirmed
2,500,000 children were vaccinated during the April National Immunization Days (NIDs) in Balochistan
800,000 children were vaccinated 126 Permanent Transit Points