The stories below highlight some ways in which women are breaking barriers, driving change and inching us closer to a polio-free world wherever they take charge – from doorsteps to laboratories to decision-making tables.
Driving regional solidarity for polio eradication
Dr Hanan Balkhy, WHO Regional Director for the Eastern Mediterranean
Dr Hanan Balkhy made history in February 2024 when she became the first woman to take up the post of WHO Regional Director for the Eastern Mediterranean. With unwavering determination, she embarked on her new role with a clear vision: to eradicate polio during her tenure.
In her nomination speech, she shared her inspiration, drawn from success stories of joint efforts across the WHO Eastern Mediterranean Region. Dr Balkhy fervently believes in the need for collective action to overcome the obstacles in the path to polio eradication.
Dr Balkhy will convene the Regional Subcommittee for Polio Eradication and Outbreaks. To champion the Region’s work to consign polio to history, she will support the regional polio eradication programme, remove obstacles and work closely with global and regional decision-making bodies.
She calls upon all stakeholders to unite with resolute determination until polio becomes nothing more than a distant memory.
Blazing a trail with the Regional Subcommittee
Her Excellency Dr Hanan Mohamed Al Kuwari, Minister of Public Health, Qatar
An inspiration to women globally, Qatari Minister of Public Health H.E. Dr Hanan Mohamed Al Kuwari has been harnessing decision-makers’ power to galvanize action for polio eradication.
As Co-Chair of the Regional Subcommittee for Polio Eradication and Outbreaks since 2022, she has created a strong sense of solidarity among Member States of the Region and partners, reminding them of the urgent need to prioritize polio eradication. Using every possible chance to highlight the challenges faced by countries with wild or variant poliovirus cases, she has mobilized action to reach vulnerable children with polio vaccines and other health services.
Dr Al Kuwari has used her platform and voice to reveal issues faced by polio eradicators in the Region and offer solutions. At the same time, she has raised the visibility of the trailblazing Regional Subcommittee’s goals and work.
KARACHI – The only life Huma Ashraf has known outside her home is of a health worker. That’s what made her step out on September 11, 2023, when she was verifiying microplans in a slum behind a railway track.
Hours later, in a moment that would redefine her life, she was rushing to Karachi’s Jinnah Hospital in an ambulance all by herself, following a train accident.
“It all happened so fast. I had to verify the homes behind the tracks and the only way to get there is crossing the railway track,” she says, recalling that day of the accident with exceptional calm. “The train seemed far away, and I thought I could cross over, but there was a gush of wind and my dupatta was caught in the train.”
In a mere matter of minutes, her life changed as she lost both feet.
The people who witnessed the accident called for an ambulance. With startling presence of mind, she collected the feet in the hope of a surgical reattachment and specified which hospital she wanted to go to.
Hina, her younger sister, is amazed by Huma’s courage that day. Showing the text message she received, she shares how Huma wrote to her with striking clarity. “Pair kat gaye hain, hospital ja rahi hun. Ammi abbu ko mat batana” (Have lost my feet, going to the hospital, don’t tell mom and dad.)
By the time Huma was taken into surgery, nearly five hours later, the damage was irreversible.
Hina worked up the courage to tell their parents about the accident after the surgery. Her mother initially thought Huma’s toes were affected. “I couldn’t fathom the extent of it,” says her mother Rukhsana.
A Legacy of Healing
Since Huma was 14, she has known what an aspirin could do, the contraceptives women would seek and that two drops of the oral polio vaccine could protect a child from lifelong, paralytic polio. These were her mother’s teachings. As she grew older, she also learnt how to administer injections. Rukhsana would ask Huma to try injections on her, consistently training her on how to provide basic health services to the community.
Rukhsana, a lady health worker, started working in 1995. As the eldest child, Huma would go along, and the mother-daughter duo would navigate the streets of Karachi, bringing essential healthcare within reach to women and children, and making friends along the way.
All of Rukhsana’s five children have worked for the Polio Eradication Initiative at some point, but it was Huma who stayed on as a frontline health worker, working in the Polio Programme as a team member and eventually rising in the ranks to become an area in-charge.
As vaccinators, there was a time when Huma and Rukhsana were one team, a team that they were very proud of. “When important people came in big cars, we were the team that would be introduced to them because everyone knew we did our job well,” Rukhsana says. “Everyone who saw Huma was amazed at how much she could walk in a day and now…I would have never imagined that one day Huma won’t be able to walk.”
“Both of us still forget what happened. Last night, someone came knocking on the door with some tea and I couldn’t find my slippers, so I asked Huma where hers were, but then I remembered that they would be somewhere on the railway tracks that day,” she adds.
Much of Huma’s nights are spent in pain, especially in the feet that are no longer there. “I think it’s the nerves, my nerves still feel the pain. I can feel my toes hurting, and then realize that they aren’t there anymore.”
Despite a life-changing loss, this is the work Huma still wants to do. “I want to return to work in polio,” she says with a belief that better days are yet to come. The accident has offererd a new level of acceptance and grace. “If God has put me through this difficult time, then I will also be given the strength to bear it.”
“My father cries a lot about this. I told him we have to accept things as they are. This has happened, Allah has put us through a difficult time. If one door closes, another one opens.”
The Bonds That Strengthen
The accident has redefined the meaning of family for Huma. The outpouring of support from colleagues and leaders in the Polio Programme has been overwhelming. For Irshad Sodhar, Coordinator for Sindh’s Emergency Operations Centre, ensuring Huma’s recovery is a mission.
“Looking after the wellbeing of frontline workers is most important. While they do this arduous job selflessly, it is the programme’s duty to support them when they face any adverse situation, especially in the course of their work,” he says.
He is a frequent visitor to the family, and Huma and Rukhsana both look forward to seeing him.
“It is my mission to ensure that Huma gets back on her feet. After the accident, I mobilized everyone we could, from the National EOC Coordinator to the Sindh Health Minister and Deputy Commissioner. We have worked to ensure the family has enough funds and the house is made disability friendly with toilets remade and all parts of it accessible for her. I am amazed by her resilience. After all this, she still wants to work to end polio,” he says, adding “Global polio eradication depends on the motivation of frontline workers. We can’t finish the job without the utmost support of frontline teams on ground.”
When Dr Shahzad Baig, the National EOC Coordinator, talks about Huma, the word that is oft repeated is of family. “Huma is one of the most remarkable people I have ever met,” he says. “We met soon after the accident and I was amazed to see how unbroken her spirit was. She only had gratitude and determination to be better. This feeling of awe stayed with me for days after I met her,” he says.
“She is the true spirit of our polio family. We will make sure she recovers completely and is able to walk on prosthetic feet. Our polio partner, Rotary, has already provided the support for the prosthesis.”
For Dr Zainul Abedin, the WHO National Polio Team Lead, Huma’s unbreakable spirit exemplifies the strength within the polio family. “Huma’s journey, marked by both loss and unyielding hope, mirrors the dedication of health workers across the country. There are many brave souls like Huma who are part of this noble mission to end polio from Pakistan,” he said.
Dr Abedin added: “We salute Huma and every frontline worker, acknowledging their sacrifices and commitment, and will continue to ensure a highly supportive environment for them.”
Huma’s journey and resilience caught the nation’s attention on October 24, 2023, World Polio Day.
In a ceremony that highlighted the relentless efforts of health workers in the fight against polio, Prime Minister Anwaarul Haq Kakar honoured Huma with a shield appreciating her services. This recognition was not just for her contributions to public health but also for her unyielding spirit in the face of adversity. Huma was unable to travel to Islamabad. Dr Baig accepted the award on her behalf and the PM vowed to bring it to her himself.
As Huma prepares for a new chapter in her life, her story is not just one of loss and hardship, but of immense strength, community support, and unwavering hope. “Things have changed, but life goes on,” Huma says with a smile. “We have to embrace it, whatever it brings.”
Huma is eager to start working for polio eradication again.
Sindh EOC Coordinator Irshad Sodhar got frontline workers from across Pakistan to send her messages, all of them expressing their belief in her and wishing for her strength. Huma had a message for them too: “You are not alone. There is a huge programme behind you, which is there for your support. Your work is greater than you think.”
Rukhsana says she has never felt as supported since she started working in 1995. “In this time, I have really felt what it means to be part of a family.”
By Zehra Abid, Communications Officer, WHO Pakistan (Video by NEOC)
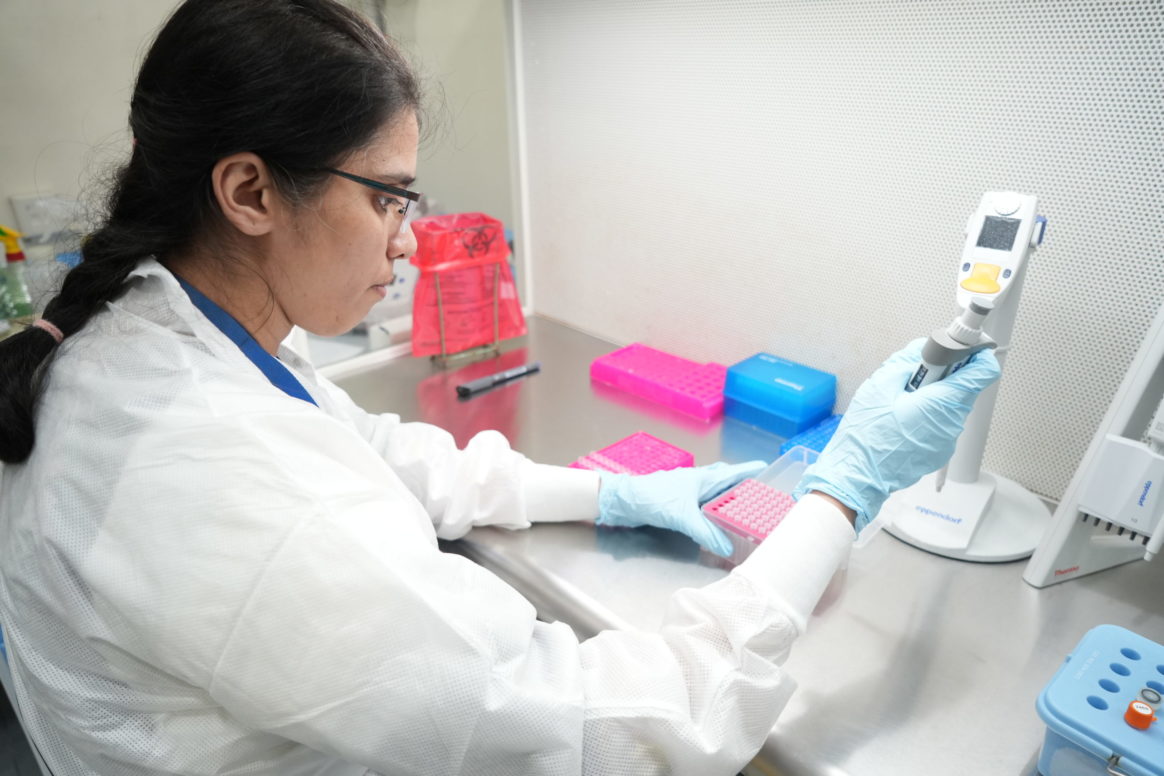
After completing her bachelor’s degree in medical laboratory science, she cut her teeth in a HIV drug resistance lab in Botswana, where she tested blood samples to determine whether a patient with HIV had a mutated form of the virus which did not respond to antiretroviral therapy.
“Once you are in the lab you realize it’s not just a job, it’s more like a calling,” she says. “Someone sends samples to you, and you are the first one to see results and ask, ‘how is this going to impact the patient, the community as a whole, and then the country as a whole?’”
In 2019, just before the onset of the COVID-19 pandemic, Mphoyakgosi was transferred to the National Health Laboratory and when the pandemic hit, she was one of the first national experts to be trained by World Health Organization on how to test for COVID-19.
This period was a career highlight for Mphoyakgosi. “COVID-19 taught us a lot. When we get outbreaks now, we have learnt from COVID what can be done better,” she says.
Currently, as part of polio prevention, she tests wastewater samples for the poliovirus. And believes firmly in homegrown excellence in her field.
“My dream for my country Botswana is to have a well-established, operationalized national public health laboratory,” she says. “I think we have capacity in terms of human resources, in terms of infrastructure. What we need now is the drive to move towards excellence. You know, embracing the science as it is and technology as it comes.”
Following the recent outbreak of Wild poliovirus type 1 in the country, she has been helping to prepare her community for a forthcoming vaccination drive, which aims to protect nearly 4 million children in the four most at-risk provinces.
Having been involved in the health sector for decades, Raquelina also spends her days encouraging other older people around her to stay active, eat healthily and to keep serving their community, just as she does.
According to the World Bank, people aged 65 and above represent only 3% of the total population in Mozambique. But Raquelina sees her age and many years of experience as an asset rather than a hindrance.
¨I am not afraid of getting old,” she says. “I feel proud because I am active, and my experience is key when it comes to contributing to the health of the people in my community. ¨
Raquelina doesn’t let her age restrict her ambitions either. “I want to go back to school and further my education,” she says. “I will keep moving forward. I will do whatever I am supposed to do. No one can take that away from me.”
Giza, Egypt, is home to the ancient world-renowned pyramids and a medical marvel of the modern age — the accredited Polio Regional Reference Laboratory (RRL) at the Egyptian Holding Company for Biological Products and Vaccines (VACSERA). Director of the polio regional reference laboratory,
Amira Zaghloul oversees five different departments, working closely with her 25-member team. They regularly conduct poliovirus diagnostic tests on stool samples obtained from children as well as sewage samples from Egypt. Additionally, they carry out sequencing of samples that have been identified as positive for polio in Egypt, Iran, Iraq, Jordan, Sudan, and Syria, which determines if the polioviruses confirmed are related to any other ones. Their goal is to meet tight deadlines, to swiftly respond to any detection of the poliovirus.
Like her counterparts across the Region, Ms Zaghloul and her colleagues rely on the latest laboratory and digital technology. With support from partners, they regularly upgrade their technology and skills to ensure the shortest possible time between sample collection and churning out results. Soon, for example, Ms Zaghloul and her team will acquire the next generation of sequencing technology – that will help test the entire genome of a virus, or genetic materials that make up a virus, and identify any mutations. This will also help to determine the origin of detected polioviruses, and track epidemiological patterns of spread.
Her work doesn’t come without challenges though. When she first took on this role, Ms Zaghloul faced negative social perceptions of being a female leader of a mixed team of men and women. To address this, Ms Zaghloul introduced rules and regulations that apply to all, regardless of age and gender.
People working in health should exemplify a spirit of perseverance, devotion, hope and ambition – regardless of their gender – she emphasizes.
When Dr Hanan Al Kindi finally settled on what to study − over virology, medicine or business — she had no idea she would need negotiation skills in her job. As the head of nine polio and measles laboratory departments that test samples from Bahrain, Qatar, United Arab Emirates and Yemen for polioviruses, Dr Al Kindi ensures everything runs like clockwork.
At times, this involves thinking out of the box. After noting huge time lags in the delivery of stool samples – used to test for polioviruses – from Yemen to Oman, Dr Al Kindi rolled up her sleeves and got to action. She learnt that after driving through mountains and deserts to reach Oman’s borders, the refrigerated trucks that transport stool samples were kept at the border for hours of inspection. Dr Al Kindi and her team got the contacts of officials at the border and invited them over for a chat.
Her determined negotiation skills and ability to read the room – to understand when peripheral stakeholders such as officials at the border and couriers needed more context about the laboratory’s role in saving children from polio — eventually helped reduce the red tape at the border. This means Dr Al Kindi and her team can test for polioviruses and turn over their results to the polio programme in Yemen in less time than before. This steers timely and appropriate outbreak response activities, including polio immunization campaigns to protect children from polio.
Dr Nayab Mahmood plays a vital role in ensuring samples are tested for poliovirus as swiftly as possible for timely interventions in Afghanistan and Pakistan – the only two countries left with naturally occurring poliovirus.
Dr Mahmood is a virologist serving the polio programme of the Regional Reference Polio Laboratory at Pakistan’s National Institutes of Health in Islamabad. Her role involves intricate technical procedures, including molecular diagnostics, and genetic sequencing of the poliovirus genome. This work helps to determine how wild polioviruses are spreading across both endemic countries.
Being part of an emergency programme means that Dr Mahmood and her colleagues need to be available 24 hours a day – a pace that is impossible to maintain without feeling an impact in one’s personal life. She feels that the best way to maintain a work-life balance is for each member of a team to communicate their needs with each other, which further helps the programme’s leaders like her to shape policies and programmes that enable a good work-life balance.
Grateful that she hasn’t had to challenge any stereotypes related to gender dynamics in her role,
Dr Mahmood credits this to directives in her workplace that support gender equality, and to the culture of her individual team. These attributes have blended to create an equitable environment where everyone can use their abilities.
Chief of the Laboratory of Clinical Virology in the Pasteur Institute of Tunis, Professor Henda Triki makes a concerted effort to share her knowledge with others. Her altruistic spirit goes beyond her laboratory, especially as her specialty of work is still rare in North Africa: She teaches virology at the Faculty of Medicine of Tunis, and constantly keeps an eye on how best to upgrade her team’s skills and technology at work.
Professor Henda Professor Triki has a collaborative leadership style at work, which results in her sharing her team-building skills with her colleagues – which has helped them address challenges many times before, including during the COVID-19 pandemic. Amidst the chaos and anxiety during the pandemic, Professor Triki and her team had strong moments of solidarity and collaborative work.
Professor Triki wants her fellow female colleagues to be proud of working for the polio eradication programme, as it offers great opportunities. It has allowed women to distinguish themselves from others by acquiring skills that other laboratories do not have. She is pleased to note now that there are many women who are the face of specialized laboratory work in the Eastern Mediterranean Region.
This year, the UN’s theme for International Women’s Day is ‘DigitALL: Innovation and technology for gender equality’.
ISLAMABAD – Poultry farming, EPI technicians, creative writing, midwifery, embroidery, online businesses: it’s a room filled with possibilities and dreams when women health workers come together to imagine their lives in a polio-free Pakistan.
These ambitions surface during the workshops the Pakistan Polio Programme initiated last year, as part of a unique project to actively listen to female frontline workers in the areas at highest risk for poliovirus transmission across the country.
The initiative used a bottom-up, data-informed approach to better understand the experiences of women on the frontlines and hear their ideas for how the programme can better support them to do their jobs safely and effectively. And came with a prior promise: leadership from all partners at the Emergency Operations Centres were to review – and implement – workable solutions.
This systematic listening process, which began in July 2022 and concluded last week, was done in two parts: First, an independent research company was brought on to conduct more than 2,600 randomized, anonymous surveys with polio frontline workers across Pakistan to understand their unique challenges and experiences in the field. After this, based on the results of these surveys, 14 workshops were designed to hear from women frontline workers themselves on what they think are the solutions to the challenges they face.
Female health workers from the polio endemic districts of Bannu, DI Khan, Lakki Marwat and Tank in southern Khyber Pakhtunkhwa to the geographically challenging terrains of Chaman, Quetta and Killa Abdullah in Balochistan to Punjab in central Pakistan to Sindh in the south of the country to the capital city of Islamabad were brought together in this series of workshops.
The workshops were also moderated by a third party to allow for open and honest discussions, and carefully curated to create spaces where, for the first time, the women were the chief guests, they were the people who mattered most, while everyone else had one job: to listen.
“When you get respect, you get everything. It’s the first time that we have talked, and other people have listened,” says Fauzia Naseem, an Area-In-Charge from Chaman.
As each of the two-day workshops finished, there was excitement, energy and almost a sense of disbelief that hours had been dedicated to listening to them. “I’ve been here since 2017 and no one has ever really asked us what we think. Otherwise we are only told where to go and what to do. Today I feel like what we say matters,” says Samreen, a polio worker, from Tank.
“This is a very special project – and a very insightful one too. It offers us the opportunity to gain from the wealth of knowledge of the polio programme’s frontline staff. For the very first time, the people who actually do the work of delivering the vaccine to a child have been systematically asked how they think it should be done. We are currently looking into their suggested solutions and seeing which are implementable and can be taken forward,” said Dr Shahzad Baig, the Coordinator of the National Emergency Operations Centre in Islamabad.
“For many women, this is the first time they are together to just talk to each other, hear from each other, take a selfie and be in a space where they have the right to simple joys that they otherwise may not have access to. The workshops for women from southern Khyber Pakhtunkhwa were particularly special. These were held in Islamabad and for many women, this was the first time they had visited the country’s capital city. Their excitement and sheer joy was infectious. It lit up the room,” said Dr Atiya Abro, Deputy Director Ministry of National Health Services.
The last session in all workshops was dedicated to listening and understanding the women’s diverse interests in other career pathways after polio, and what skills or support the workers felt would be needed for them to transition into these jobs in the future.
This initiative was coordinated by the Pakistan Polio Programme’s National Gender Group, comprised of representatives from the government and partner agencies including WHO, UNICEF, BMGF and N-STOP.
“Having the opportunity to listen and give center stage to these women has been a true privilege. It’s encouraging to see such strong commitment from Pakistan programme leadership to support these female health workers – not only in their work toward our collective goal of eradicating polio, but also to facilitate transitions into other potential livelihood opportunities in the future. We look forward to the next phases of this exciting initiative as well,” said Sang-Hee Min, Senior Programme Officer, Bill & Melinda Gates Foundation and member of the National Gender Group.
“Polio teams are a valuable asset to our country,” said Dr Baig. “It is very important to me that when we finish polio from Pakistan, we don’t just pack up and leave but utilize this incredible workforce. We build systems and create opportunities to serve the workforce, a majority of them women, and find some way, however small, in giving back to the people who have worked tirelessly to protect the children of our country.”
By Zehra Abid, Communications Officer, WHO Pakistan
As an epidemiologist in Iraq with 25 years’ experience eight of which were in immunization, Dr Israa Tariq Mahmoud is responsible for providing vaccines to all health centres and institutions that work within the Rasafa District of Baghdad. She also follows up on the availability and distribution of vaccines to ensure they reach children across the area she covers.
Dr Israa chose to work in immunization as it would allow her to build relationships with the children and families in her community. She feels a strong sense of social justice in her efforts to ensure that all children, regardless of their social status, have equal access to vaccination.
She adds that she and her colleagues who are health care workers are all cogs in the chain of efforts required to eradicate polio, from surveillance to vaccine follow-up. That follow-up includes checking that children have taken all doses of the vaccine and monitoring for any adverse events following immunization (AEFIs). They also conduct disease surveillance as they visit children’s homes.
Dr Israa says she feels the same drive a parent or caregiver does when they look after their own child. She has advice for health workers, especially young ones: “We all, males and females, have a role, no matter how small, in building our country.”
Defying norms take guts – which Shiza Ilyas has no shortage of. Ten years ago, she joined Pakistan’s polio eradication programme in Lahore as a vaccinator to support her family after her father, the main breadwinner, passed away. Going from one door to another, talking to families, and protecting children from lifelong disability has brought her both purpose and peace.
Shiza is the first woman to serve as Area-in-Charge in Lahore. Responsible for running vaccination campaigns in Lahore’s Union Council 44, she is well known and respected among her peers. More extraordinarily though, she carries out her vaccination duties on a motorbike – a rare sight in Pakistan.
When Shiza expressed interest in serving as an Area-in-Charge, her supervisor chuckled and said no woman in Lahore had ever wanted to take on this role before. At the very least, he said, she would need to be on a motorbike to travel long distances and check on polio teams.
With support from her grandfather, and eventually her mother, and with riding instructions from a cousin, Shiza was soon whizzing through the streets, after a quick stop at her supervisor’s office.
Shiza’s work involves supervising polio campaigns in her area and checking in on teams during the day as they go from house to house. She tallies their data and at the end of the day, if any children have been missed, she personally visits their houses and vaccinates them.
“I never paid attention to negative comments from anyone about being a woman on a bike,” she says. “I always believed in myself and did what I wanted to do.”
“When you put polio drops in a child’s mouth, you feel happiness inside, happiness that you have saved a child,” she says. “I urge people to come and work for this feeling. This work brings a lot of peace.”
In Djibouti, every day, Houda Houssein Okeih vaccinates people who visit the health facility where she has been working since 2015. During polio vaccination campaigns, she focuses her efforts on children under five years of age.
Working with parents, mothers, and their children on a daily basis has made Houda a popular figure in the neighbourhood. With 20 years of experience as a nursing assistant, Houda is known for her outspokenness, clarity and passion for engaging mothers. She makes a point of ensuring that parents know and follow vaccination schedules and keep records. Sometimes, she needs to pester them a little, she adds, laughing, so that parents take timely vaccination seriously.
Houda enjoys being among the community. To follow up with her patients, she often scouts the neighbourhood, similar to a detective, to look for families who haven’t followed their children’s vaccination schedule. She then directs them to her health facility, to encourage them to vaccinate their children and give them a healthier and brighter future.
Inspired by a television programme
Over in Afghanistan, Farida* is a vaccinator who is pleased to be serving her community through polio campaigns.
Farida feels lucky to be contributing to eradicating polio. The best part of this job, she says, is that she can see the impact of her efforts to prevent Afghan children from becoming paralyzed. In 2022 to date, just two children have developed paralytic polio in Afghanistan.
Farida was inspired to work as a vaccinator after she watched a television programme that depicted children paralyzed by polio. The story of these children’s lives and struggles resonated with her and gave her a sense of professional purpose.
In efforts to support women like Farida to play an important role in polio eradication, the GPEI in 2019 endorsed a Gender Equality Strategy. It also aims to promote the integration of a gender perspective into programming, and to support countries to address gender-related barriers to vaccination.
In WHO’s Eastern Mediterranean Region, the polio eradication programme is working on addressing gender-related barriers to vaccination of children and surveillance for poliovirus. To this end, two Technical Advisory Group (TAG) meetings recently conducted for Afghanistan and Pakistan, the countries where the wild poliovirus is still endemic, also provided guidance on integrating solutions to gender-related barriers into eradication efforts.
Mounting speedy responses by rapid testing
When she was young, Dr Nabila Mohammed Al Moalimi dreamt of being a pediatrician. But when her father was misdiagnosed and given the wrong medical treatment, she decided to play a role in strengthening her country’s laboratories. Now, Dr Nabila serves as the Director of the Molecular Biology Department in Sana’a, Yemen.
After a two-week training session in a polio laboratory in Pakistan, Dr Nabila and a colleague returned to Yemen to start up a new laboratory division in the Ministry of Health’s Central Public Health Laboratory, Sana’a. This will solve a major problem for the polio eradication programme in Yemen.
Previously, the polio laboratory in Sana’a would collect polio samples and ship them to the Regional Reference Lab in Cairo, Egypt, for testing – all with no delays. But after the war broke out, stool samples had to be sent to the KEMRI laboratory in Nairobi, Kenya. The return of results could take up to three months – a costly delay that could exacerbate the spread of polio outbreaks.
During her mission to Pakistan, Dr Nabila and her colleague were trained in conducting rapid tests to flag polio infection in stool samples before sending them to a laboratory from the WHO-accredited Global Polio Laboratories Network for poliovirus diagnosis. In the event a sample tests positive, the team can now immediately alert technical experts and health authorities to plan a response. This response can include testing samples from contacts of the child who tested positive for polio, and vaccinating children to boost their immunity in affected locations. This response, especially when done quickly, prevents further spread of polioviruses.
Thanks to the expertise of Dr Nabila and her colleague, alongside several others, the polio laboratory in Sana’a may soon be able to perform direct detection of poliovirus from stool samples. They can also tell whether a polio virus is wild or a variant type, which informs an appropriate response.
A polio worker administers the oral polio vaccine to a child in Karachi. Credit: @SalmanMahar
Polio is one of the world’s most devastating diseases. It mainly affects children under five and in one in 200 cases it results in lifelong paralysis. Amazing progress has been made in fighting polio globally: according to UNICEF, there were a reported 20,000 children paralysed by polio in Pakistan in 1994. By 2021, new paralysis cases had dropped to just one child. However, as long as just one child remains infected, all children are at risk.
Identifying and reaching unvaccinated children has been a challenge, but big data startups like Zenysis, in partnership with Pakistan government partners, are making inroads.
Vaccination data is only useful if it’s accurate
Abid Hasan is the project manager for Zenysis – a Gavi INFUSE pacesetter since 2017 – in Pakistan, and he explains the barriers to a more effective vaccination programme in the country:
“Data is like people, in that if data sets don’t talk to each other then they won’t work well. Zenysis gets data and data sets talking.”
Community health workers employed through Pakistan’s Polio Eradication Programme and the Expanded Programme of Immunisation go door to door to collect vaccination data, sometimes using datasheets, sometimes paper, sometimes recording data through WhatsApp. It can be difficult to track families with no formal address, or mobile communities with no fixed address. With 14 million children requiring a polio vaccination every two months, recording accurate data is a mammoth task.
The resulting data can be imperfect, with duplication a particular challenge. This is where Zenysis’s platform comes in. Zenysis software integrates, de-deplicates and harmonises more than 20 siloed datasets, including polio data, immunisation registries and population data.
Combined, the data can be used far more effectively for analysis and, importantly, action on the ground. The result? A new and improved vaccination plan, personalised for each vaccinator’s district – known as a microplan.
A Community Health Worker goes door to door during the August polio campaign to give children the oral polio vaccine. She finds a newborn zero-dose child and records that data into her register. Credit: @SalmanMahar
Microplans help health workers target zero-dose children
The enhanced microplans provide health workers with granular information on each child in a region, including their vaccination status, age and address. This information can be used to identify individual children and highlight neighbourhoods where there are clusters of unvaccinated (zero-dose) children. This in turn means better use of time and energy, and better outcomes for communities.
The effect, explains Hasan, is seen in three key areas. “Firstly, the newmicroplans give community health workers the real picture. Second, frontline workers now have a plan to follow and are no longer using broad or inflated data that is hard to actionize. Third, this approach is measurable – when you reach a target, that goes into the system. With accurate data, you can really see the impact.”
Health workers on the ground have seen the difference. Sadaf, a community health worker for Polio, in Karachi, says: “Before the microplans the vaccinators were given a long list of children with duplicate entries in them, and they were extremely difficult to track. After receiving these microplans we can easily decide where to set up our outreach sites and mobilise children to bring them there for vaccination in a systematic manner.”
The impact has been impressive. Since January 2022, the Expanded Programme on Immunisation in the Sindh region has used the Zenysis platform to identify over 28,500 true zero-dose children in the region and vaccinate 12,724 of them with the aid of microplans. In March to June of this year, 3,854 zero-dose children were vaccinated with the help of the new microplans in the regions where they have been implemented.
Community Health Workers using Zenysis provided microplans to identify houses with zero-dose children in high risk areas of Karachi. Credit: @SalmanMahar
Gavi support has been vital in creating goals and driving change
Zenysis was part of Gavi’s INFUSE programme, which connects high-impact innovations with the countries that need them most. Hasan explains that for countries like Pakistan, the investment from Gavi is vital to enhance healthcare budgets, but also to help provide momentum and set goals for vaccination programmes.
Looking ahead, Zenysis is collaborating closely with government partners to expand the platform and vaccination approach throughout Sindh province, tackle other vaccine-preventable diseases, and improve the government’s technical platform management capacity.
As Hasan says, “Not everyone is a data expert – but if you can go on a platform, go into a dashboard, and see all your data into one workspace then you can reach a zero-dose child and their family, and get them vaccinated.”
And with each child vaccinated, we get a step closer to a world where infection by wild poliovirus is a thing of the past.
In 2021, when the news of cancer hit, Nomina Akhtar felt her world collapsing. It was discovered too late. By the time she knew, it was already stage-3 breast cancer.
Since 2015, Akhtar has been part of Pakistan’s polio programme as a community health worker. During these six years, she has found friends and well-wishers among her team members who have given her the support to carry on.
Akhtar, 43 and a mother of three continues to work for polio eradication as she undergoes treatment for cancer. “I gathered my courage and promised that I will fight till the end and live for my children. All my family, colleagues and seniors were with me whenever I needed support. That gave me courage and made me believe that I could, in fact, beat cancer.”
Based in Peshawar, Nomina’s husband and her three children, aged six, seven and 18, rely solely on her income. The lockdowns due to the pandemic caused her husband, a motorcycle mechanic, to close down his shop that has yet to reopen.
A life with cancer has been both physically and emotionally exhausting. She is undergoing both radiation and chemotherapy in Peshawar. This means a commute of almost 20 kilometers after a whole day of work.
“When I have to go for chemotherapy after work, it becomes very draining. I have to take public transport and wait at the hospital for hours. There are times when I have to return without treatment because either the machine is faulty or something else comes up. This treatment regime along with the medicine will continue for at least five years. It’s excruciatingly painful,” she says.
Polio programme: a great source of strength for Akhtar
“My colleagues are like my extended family, and I am like a sister to them. When I found out about my cancer, they wept with me. They have stood by my children and myself every step of the way.”
The supervisor of her area, Uzma Mansoor, says that when they first heard the news, they were devastated. “But it’s great to see that she has not lost hope and is fighting the disease like a champion,” she said.
The community she works in has also been incredibly supportive. “Some of the people in my work area came to know about my illness and they appreciated the fact that despite fighting cancer, I come to their doorstep during every polio campaign. Irrespective of extreme temperatures and illness, I am there to vaccinate their children and protect them from this life-threatening disease. Their support has increased manifold after this.”
Sahibullah, the Union Council Polio Officer of her area, says not only does Nomina continue to vaccinate children, but she is a role model for all other polio workers.
“It was God’s will, and we will face it with courage,” says her husband Aurangzeb Akhtar. “Despite being ill, Nomina is the one who keeps us going. She is working and earning for our family as well as motivating us to not lose hope. My children and I are so proud of her. Inshallah she will get well very soon.”
Nomina has strong conviction. She is fighting cancer and polio simultaneously, and is determined that she will defeat both very soon. “At least cancer has treatment,” she says. “Polio is incurable and the sooner we end this disease forever, the better.”
By Mohammad Shoaib, Provincial Communications Officer KP, WHO Pakistan
This International Women’s Day, we get to meet some of the women leading the polio eradication efforts in Pakistan.
On International Women’s Day, Spanish Minister for Foreign Affairs, European Union and Cooperation and Gender Champion for Polio Eradication, José Manuel Albares pays tribute to all the women in polio eradication across the world and reminds us that women are still underrepresented in senior leadership and decision making roles in global health and that these gaps in leadership are driven by stereotypes, discrimination and power imbalances that we are all responsible to tackle.
GPEI announced a series of commitments to advance gender equality at the Generation Equality Forum in Paris, organized by UN Women and hosted by the Governments of France and Mexico between June 30 and July 2, 2021. The Forum kickstarted a 5-year journey to accelerate ambitious action and implementation on global gender equality.
Through its new Eradication Strategy 2022-2026, the GPEI committed to integrate a gender perspective into programming to support countries to address gender-related barriers to polio vaccination, to increase women’s meaningful participation and decision-making across all levels of the program, and to utilize gender-sensitive indicators to ensure girls and boys are reached equally. This will be realized through policy, programmatic, advocacy and financial commitments with the goal to eradicate polio through a gender lens.
GPEI joins the World Health Organization (WHO)’s ambitious and bold commitments for gender equality and the empowerment of women and girls in all their diversity, announced during the Generation Equality Forum. The GPEI looks forward to working with a broad range of partners to deliver not only on polio eradication, but also on gender equality, for future generations.
Even long before the GPEI was formed, Monaco played a leading role in early initiatives to develop a polio vaccine. In the 1950s, Her Serene Highness Princess Grace was an advocate for the National Foundation for Infantile Paralysis in the United States of America, founded by President Franklin D. Roosevelt (himself a polio survivor).
The Foundation became known as the “March of Dimes”, so called because of its far-reaching call for funds to research a cure for polio, which at the time was one of the most serious communicable diseases in the USA. Grants from the NFIP facilitated the work of researchers such as Dr. Jonas Salk, creator of the first successful vaccine against poliovirus. But it also facilitated the work of unsung heroes, such as Dr. Leone Farrell at the University of Toronto’s Connaught Medical Research Laboratories. Farrell devised the “Toronto method” for mass production of vaccines, which made the massive field trials of Salk’s vaccine possible, paving the way for the mass vaccination campaigns which have brought us so far in eradicating polio.
Farrell is one of thousands of women past and present at the forefront of the GPEI. The role of women in polio eradication is supported by Polio Gender Champions, who work to raise the voices of women engaged in the programme, and keep gender equality high on the global public health agenda.
And today, Monaco’s proud tradition of support for gender equality and polio eradication continues, with the announcement that H.E. Ms. Carole Lanteri, Ambassador and Permanent Representative of Monaco to the United Nations Office at Geneva will become the newest Gender Champion for Polio Eradication. The Ambassador, formerly co-chair of the GPEI’s Polio Partners Group, explains the significance of this new role:
“As the Covid-19 pandemic continues to affect our lives, women pay a higher price with regressive effects on gender equality. If gender dynamics are not taken into consideration, polio interventions will not be as effective, with the potential risk of exacerbating existing inequalities. More than ever before we must advocate for a meaningful inclusion of women in decision making processes and adopt policies in health programming to reflect this. Today my commitment to these causes is even stronger thanks to my new role as Gender Champion. Following in the footsteps of Princess Grace and taking forward Monaco’s longstanding commitment to gender equality and polio eradication, I am determined to use my voice to advocate for gender mainstreaming in polio eradication to reach every last child.”
Ambassador Lanteri joins the ranks of other gender champions striving to raise awareness of the role of women in polio eradication and on the importance of addressing gender related barriers to immunization. Their work will be instrumental not only in eradicating polio, but also in creating a legacy for recognizing and empowering the role of women in major public health initiatives.
Anisa’s story epitomizes the heroic contribution of women polio workers in Afghanistan who continue building trust in vaccines among parents and caregivers in the quest to immunize every last child and end polio.
The yellow taxi drives slowly on an unpaved Afghan road. It has rained heavily turning the detritus on the ground into a muddy quagmire, and the car labours in its efforts not to get stuck.
Stopping near a house, a young woman in a black scarf and traditional dress climbs out of the car. This woman is Anisa, a UNICEF consultant for the polio programme. Today she is visiting parents who are refusing to let their children be vaccinated, to explain why the two drops of oral polio vaccine (OPV) are critical for their health and wellbeing.
We enter one of the houses and meet an elderly woman.
“I am not vaccinating my grandchildren!” The woman sounds resolute, but we stay anyway. “Can we talk about something else?” Anisa asks calmly. Shortly thereafter, we’re drinking tea and praising the mild weather. The grandmother tells us her left leg was almost fully paralyzed half a year ago and she can’t walk normally.
“This is horrible. You should go to the clinic. I can recommend a good doctor for you. And do you also know that children who are not immunized can also be paralysed because of polio?” Anisa starts getting to the point of our visit. “You have two wonderful granddaughters and it’s easy to protect them.”
The grandmother doesn’t seem convinced but asks questions about the rumours around the vaccine. Anisa explains that OPV is safe, halal for Muslims, and it is the only way to protect children from getting polio. One hour later, the grandmother nods – she finally agreed to vaccinate. It is hard to say what was the turning point that convinced her. Maybe the photos of paralyzed polio survivors that Anisa showed her on her phone; maybe information that polio vaccination is required for Hajj and Umrah (religious pilgrimages to Mecca which must be done at least once in lifetime by all Muslims); or simply the fact that Anisa vaccinated her own two children, and they are safe and well. The fact that the grandmother finally agreed to vaccination feels like a big victory – but it’s just a small step in the battle against polio.
Anisa has been working in the health sector for almost 10 years – as a midwife, female mobiliser vaccinator, nutrition officer and a clinical mentor. She first started to support the polio programme as a Provincial Communication Officer (PCO), supervising over a hundred communication cluster supervisors.
During the national immunization campaigns, even during the COVID-19 pandemic, Anisa supports the teams by conducting information sessions for refusal families and arranging discussion sessions for community groups. She also holds awareness raising sessions on how to prevent the spread of COVID-19.
“After my first day working with refusal families, I wanted to leave the job. I didn’t convince anyone. But then I managed to convince one family with five children, who have never been vaccinated and it felt like such a victory that I decided to stay,” remembers Anisa. “Now I know how to approach different people; I understand what type of information is important to persuade them to make the right decision.”
Therese and Léonie reminded me of this hard truth in a recent visit to a hospital in N’Djaména, Chad. One is a newborn girl and the other is a veteran of the campaign to eradicate a human disease for only the second time in history –polio-.
As a Gender Champion for Polio Eradication, I have committed to supporting the global initiative to eradicate polio and the women who work tirelessly to protect children from lifelong paralysis. During my visit to Chad, I had the honour of giving two drops of life-saving oral polio vaccine to two newborns.
Protected from a disease which once struck millions of children, Therese now has a better chance of a healthy life. Thanks to the Global Polio Eradication Initiative (GPEI) – spearheaded by Rotary International, national governments, the World Health Organization, UNICEF, CDC, the Bill & Melinda Gates Foundation and Gavi, the Vaccine Alliance – she is one of more than 2.5 billion children who have received the oral polio vaccine, as the global polio caseload has been reduced by 99% since 1988.
But as I looked at Therese, I also wished that she would have a better chance not just for health, but also for opportunities to prosper. I thought of a recent WHO report I had read – Delivered by Women, Led by Men – which observed that women make up 70% of the global health workforce but hold only 25% of senior roles – a situation that is no different for the polio program. Would Therese’s future reflect that disparity?
I found both frustration and hope in answer to my question when I listened to Ms. Léonie Ngaordoum, the woman responsible for the campaign which brought the vaccine to Therese.
Léonie is head of vaccine operations for Chad’s immunization programme. It is women like her who have brought us this far in the long fight against polio. It is women like her who have gone the extra mile to keep their countries safe when, in 2020, the polio programme faced unprecedented challenges in the face of a new pandemic- COVID-19.
Her journey to a senior public health position in Chad has been difficult. Driven to remote areas on dangerous roads to oversee vaccination campaigns, she has twice suffered accidents, one of which left her with severe spinal injuries. She has faced gender discrimination, countered vaccine misinformation, convinced vaccine sceptics, and stayed the course despite the severe strain of COVID-19, and struggling for respect and recognition in a male-dominated environment.
Today she has a clear vision to share: “I speak about vaccination as if it were a vocation…the program change needed to achieve polio eradication is to empower enough women.” Léonie’s experience highlights the necessity of increasing senior roles among women in the health workforce and involving them in policy decisions.
Women like her frequently operate in dangerous and conflict-affected areas, putting their own personal safety at risk – all in efforts to protect communities from deadly diseases. Women have a greater level of trust with other women and thus are able to enter households and have interactions with mothers and children necessary to deliver the polio vaccine. And this way they can also provide other services, such as health education, antenatal care, routine immunization, and maternal health.
The knowledge and skills gained by this workforce are already being deployed against COVID-19, in surveillance, contact tracing, and raising public awareness. Indeed, more than 50 percent of the time spent by GPEI health workers is already dedicated to diseases and threats beyond polio. It’s clear that the future of public health is inextricably linked to the status of women. Their heroic actions provide nothing less than a blueprint for the future of disease prevention. The Resolution on “Women, girls and the response to COVID-19”, adopted last year by the UN General Assembly, should play a key role when addressing these challenges and the specific needs of women and girls in conflict situations.
The centrality of women to the success of public health projects has for too long gone unrecognised, and must be formalized. That is why today, on International Women’s Day, we must pay tribute to the tremendous contribution of women like Léonie around the world in protecting their communities from deadly diseases such as polio. But at the same time, thinking of the world in which Therese will come of age, we need to commit to empower every woman and girl. It will not only make for a more just world – but a healthier one too.
Throughout her career as a Resource Mobilization Officer for WHO’s polio eradication programme, Heather Monnet has held onto her vision of a polio-free world. A respected communicator with a deep understanding of the polio programme, she was one of the first in the programme to realize that considering gender is crucial to defeat the poliovirus. Since 2017, she has successfully “led from behind”, supporting the Global Polio Eradication Initiative (GPEI) to develop a gender strategy and workstream which has become a model for other United Nations programmes, and which is designed to overcome some of the most intractable challenges facing polio eradicators.
Describing her motivation, Heather describes “putting on her gender glasses”. She explains, “We had reached a point where it seemed like we had turned nearly every stone to eradicate polio, and yet we had not defeated the disease. At the same time, the introduction of the sustainable development goals had led to an increasing awareness of gender. I began to think more about how gender affects health and health-seeking behaviors.”
“I was not, and am still not a gender expert, but as Member States began to speak more about this issue, it was increasingly on my radar. Putting on my “gender glasses”, I realized that gender was an unexplored intersection for polio eradication, and it could be transformative for our work.”
In polio eradication, areas where gender intersects with health delivery include exploring whether boys and girls are equally as likely to receive the polio vaccine, and if gender norms impact whether mothers are able to take their children to health centres for routine immunization.
In some places, such as in Nigeria, women are often more effective at delivering the polio vaccine than men, as it is more culturally acceptable for them to interact with mothers and enter homes to vaccinate the smallest children. The GPEI Gender Technical Brief showed how the presence of female health workers in Pakistan has been associated with substantial increases in tetanus vaccine coverage, attended births, and full immunization coverage of children.
To explore and respond to the gender dynamics of polio eradication, the GPEI has published a comprehensive gender equality strategy. A dedicated gender analyst works in the polio programme at WHO headquarters, and gender focal points have been appointed at regional levels and in some country offices. Data is now routinely disaggregated by sex, and there has been a concerted effort to use gender analyses to inform programme policy. The team are currently engaged in implementing the GPEI gender strategy as well as supporting efforts to mainstream gender across WHO, including through a dedicated gender data working group.
Advocating for consideration of gender within the programme has not always been easy. Heather explains, “The polio programme is huge and so many people are involved. Encouraging people to put on their ‘gender glasses’ even for five minutes can be a challenge. But what is really encouraging is that once we educate people about how gender impacts their work, they often have an “aha” moment.”
“The next and crucial steps are striving to ensure that the gender strategy is implemented. This requires all those involved in polio to be engaged – whether it’s designing a gender-inclusive microplan, collecting sex-disaggregated data during a campaign, or considering how gender impacts the way we pay vaccinators. As we integrate gender into our work, we also need to identify the building blocks to ensure that this workstream is sustainably mainstreamed. This is not dependent on one person – rather it takes everyone having exposure.”
Polio Gender Champions
The GPEI gender workstream is supported by Polio Gender Champions, who work to raise the voices of those engaged in the programme. Champions include Senator Hon Marise Payne, Australian Minister for Foreign Affairs and Minister for Women, Wendy Morton, Minister of European Neighbourhood and the Americas at the Foreign, Commonwealth & Development Office in the United Kingdom, and Arancha González Laya, who is the Spanish Minister for Foreign Affairs, European Union and Cooperation.
Heather explains that the vision and leadership of the gender champions is crucial for achieving change. “The gender champions amplify the voices of those who don’t have a megaphone on the global stage and whose voices need to be heard. For instance, female frontline workers have a lot to say, but their voices aren’t always listened to. Our gender champions raise up these voices from the field.”
“This feeds into our attempts to improve the way that health is delivered. We know that most healthcare is delivered by women, but the systems to deliver it are designed by men. Practical steps to support women employed by the programme may include ensuring that polio vaccination training materials can be understood by individuals with lower literacy, and ensuring that there are safe, private bathrooms available for women to use during long campaign days. When we plan routes to deliver vaccines from house to house, we should consider that women might prefer to take a different route which gives them a greater feeling of personal security. Women may not feel comfortable speaking about these issues to a male supervisor, so we must also ensure that enough female supervisors are recruited and trained. Gender champions are key to keeping these issues high on the global agenda.”
Over the last few years, the GPEI’s gender work has been recognized in multiple high-level forums, and is leading the way for other programmes. Heather identifies two moments when she felt particularly proud – when the Polio Oversight Board adopted and endorsed the GPEI gender strategy, and at a high-level meeting hosted by the Government of the United Arab Emirates in advance of the Reaching the Last Mile Forum in November 2019, during which the Canadian representative described GPEI’s gender strategy as one of the strongest in global health and noted that it should stand as an example for others.
Heather explains, “I have been inspired by what we have achieved – we have planted the seeds and the soil is now being nourished. Our work on gender is growing into something amazing – and the world is watching what it will become.”
Henrietta Lacks was diagnosed with cervical cancer in 1951, at the age of 31. Doctors in Baltimore, USA took a small sample of her tissue during the treatment to remove her tumour, without her knowledge – a not uncommon way to treat minorities at that time. Up to that point, attempts to grow human cells outside the body had failed. However, Lacks’ cells were different: they were able to divide and replicate indefinitely. These cells became the source of the HeLa cell line – one of the most important cell lines in medical research – and contributed to developing the first polio vaccine. While the world has benefited greatly from Henrietta Lacks’ cells, the unethical use of her cells raised concerns about longstanding medical racism towards marginalized or minority communities – and has contributed to the movement towards more people- and community-centred care.
Margaret C. Snyder is often called the UN’s First Feminist. Her pioneering career refocused the mechanisms of global development aid to include women. As she wrote last year: “There was a failure to realize that the most serious problems of development defy solution without the involvement of women.” When she began working at the UN, in the early 1970s, most women did secretarial work. Under her influence, that began to change. By 2021, women make up a significant portion of UN professional staff, and applying a gender lens to the UN’s work has become essential. This thinking was foundational to the systematic adoption of gender-based planning that has underpinned polio eradication. Margaret C. Snyder died earlier this year at the age of 91.
Dr. Folake Olayinka has spent over 20 years working in public health, including at the frontline of efforts to eradicate polio and strengthen immunization.
“At local levels, where the rubber meets the road, we need to make things work. Frontline health workers should be supported with tools that meet their needs, and training that truly values their insights, local innovations and problem solving,” said Dr. Olayinka.
Today, as a global health leader and former John Snow, Inc. (JSI) Project Director for the USAID-funded MOMENTUM Routine Immunization Transformation and Equity Project, she continues to exchange lessons and innovative strategies from the frontlines with other parts of the world impacted by polio and low immunization coverage.
On August 25, 2020, Nigeria, previously the last stronghold of endemic wild polio in Africa, was officially declared free of wild poliovirus. One of the factors contributing to this success was the ability to provide high-quality capacity building and support to improve health workers’ competencies at all levels of the health system.
“The health workers on the frontlines – particularly the community-based workers, many of whom are women – are the backbone of all of these efforts. They operate under incredible circumstances to ensure that their communities have access to life-saving health services,” said Dr. Olayinka.
Dr. Olayinka began working on polio in 2002 in Nigeria. She worked closely with colleagues at the Nigerian Ministry of Health, the World Health Organization, the EU and UNICEF to ramp up health worker training in support of the Nigerian government’s National Program on Immunization.
Her team’s dedication was remarkable. “We were willing to go everywhere to reach the last child. Once I walked four hours to support an immunization team,” she recalls.
Shaking things up
Dr. Olayinka emphasized training quality and the use of feedback to continuously improve the training experience for health workers. She led the development of numerous training guides and materials for polio eradication and developed the country’s first Basic Guide for Routine Immunization Service Providers. She also worked closely with WHO and EU colleagues to develop the first measles campaign field training materials in Nigeria.
Knowing that training of health workers must be continuous, she introduced mentoring as an important post-training approach in Nigeria’s immunization program.
“We needed to move people towards a more interactive approach,” said Dr. Olayinka. “These approaches transfer knowledge while maintaining dignity and recognize that people in the global South have something valuable to contribute.”
Recalling her experience training different types of health workers and trying to promote adult learning methods, she said, “I once walked into a room of senior health commissioners from all over the country. The room was filled with the usual PowerPoints, and people were not engaged – even sleeping.”
“When I went to the front of the room for my session, I introduced myself using my first name and explained the more interactive approach that I was proposing for the training. At first people were silent, but as the training went on, they really came alive. They were engaged and now identifying the real issues and generating the types of ideas that could truly change policy and improve services – you could see their passion coming through. I felt the ship took a turn.”
Dr. Olayinka also tackled training needs at the community-level and strongly promoted the use of local languages in the training of frontline health workers, particularly social mobilizers for polio eradication.
“At local level in northern Nigeria, most people spoke Hausa; however, training materials were largely in English at the time, and many of the women who were able to enter the homes to provide polio vaccinations did not understand English.”
“The polio programme was at a crisis point and was also facing a lot of refusals. As people in the region were not receiving other basic health services, they began not to trust polio vaccination efforts as it was one of the only services they were receiving.”
A pivot was needed, with a closer examination of what was working – and what was not – for all aspects of the eradication effort.
“These women were looking for the basics: how do I answer questions from caregivers, how do I provide polio drops, how do I enter my data?” remembers Dr. Olayinka “With this insight, I developed a flip chart using pictures – I even included a photo of my own son receiving the oral polio drops. We also used the local languages, role play, peer to peer methods, and songs as part of the training methodology.”
In the area of routine immunization, Dr. Olayinka worked with her team and other partners to introduce a stronger supervision system. The system included a checklist with clear standards for supervision of routine immunization, as well as a checklist on training quality as part of the pre-campaign preparedness. This helped National Primary Health Care Development Agency staff to provide ongoing support and mentorship for health workers. Many of these approaches and materials are still being used today and are updated periodically.
At the heart of the response, you will find a woman
Dr. Olayinka worked in a particularly challenging environment in northern Nigeria. “There are gender dimensions tightly linked with socio-cultural and deep-seeded religious beliefs in the northern state”, she recalled.
Oftentimes mothers had to seek permission from their husbands before they could allow the children to be vaccinated or access health services. “Even when they understood the value, women did not have decision-making power.”
The polio programme was able to reach women in new ways. Men originally started out as polio workers, but it quickly became apparent they were missing children under five because they were not allowed into homes due to cultural norms. The solution: hire women to go door-to-door and reach populations being missed.
“The polio programme brought women out into the workforce in an unprecedented way, says Dr. Olayinka. “Women were powerful mobilizers, particularly older, respected women and could enter any home. The polio programme was one of the first programmes bringing the women out, training them how to speak to other women and community members, which gave them a standing in the community. They also received some stipends which empowered them a bit financially.”
Many of these women later transitioned to supporting broader immunization and other health efforts in their communities, leading to higher child survival rates and less disease in communities.
“This is part of my passion when I talk about integration – these women in the communities, after getting a start from the polio programme, can be trained to talk about routine immunization, use of long-lasting insecticidal nets to prevent malaria, breastfeeding, WASH etc.”
“As a result of the polio programme they have social capital that can be expanded to improve health outcomes in their communities.”
To women leaders of the future
Dr. Olayinka remains committed to elevating the contributions of frontline health workers operating in challenging situations across the world.
When asked what advice she would give to women beginning their careers in public health, Dr. Olayinka said, “Be persistent and do not give up on your dreams. Even where you face discrimination because you are a woman, be focused and persist. Ensure that you are constantly building your capacity and equip yourself.”
“Women at all levels can make a difference, so take the leap—there are no limits to what you can achieve.”
From her first polio vaccination campaign in 1997 to the present day, Dr. De Sousa has never lost her passion for increasing access to immunization. The National Expanded Program on Immunization (EPI) Manager for Angola, she remembers her first impressions of the country, “At the time, I could see that most children in the country were not vaccinated and I was excited to help them.”
From the outset, she knew that taking on polio eradication would be challenging. “Angola had just emerged from an armed conflict and there were areas that were very difficult to access, due to dilapidated roads, broken bridges and mining activity, and for that reason there was low routine vaccination coverage. Nevertheless, I felt that I had a duty to fulfill for our children, so I accepted the challenge.”
In 1998, Dr. De Sousa was appointed by the National Directorate of Public Health to help implement the Epidemiological Surveillance System for Acute Flaccid Paralysis (AFP) – one of the primary symptoms of polio. It was a position that required grit and resilience.
She explains, “This was a big responsibility because highly sensitive surveillance for AFP, including immediate case investigation and specimen collection, are critical for the detection of wild poliovirus. AFP surveillance is also critical for documenting the absence of poliovirus circulation for polio-free certification.”
“One of my most vivid memories of the programme is from 1999 when I was trying to reach conflict-affected areas after a polio epidemic had registered more than 1190 cases and 113 deaths. I was early in my career with only two years of service and the sheer number of cases and deaths led me to be proactive and persistent in my day-to-day activities toward the eradication of the disease.”
“Another standout moment occurred on the second time that I went to coordinate a vaccination campaign in the province of Moxico; one of the vehicles in our convoy triggered a mine, so we were forced to stop the vaccination campaign as our colleagues were stranded in conflict zones for a few days. This incident captures the difficult circumstances we were operating in as health workers.”
Eradicating wild virus in Angola
For years the polio team worked to improve operations to detect polio and deliver vaccines, but the virus fought back. After registering a last case of indigenous wild poliovirus in September 2001, Angola recorded four successive outbreaks imported from India and Congo. Dr. De Sousa remembers that this caused many people to doubt that the eradication of polio would ever be possible.
“But I refused to be discouraged. I’ve never backed down from a challenge and I don’t plan to soon.”
After years of work, Angola finally received wild polio-free status in November 2015. Dr. De Sousa describes it as her proudest moment.
“I felt that I made a great contribution to my country and our children as the person managing the Extended Program on Immunization in Angola.”
A new challenge
In 2019, Angola’s immunization team faced a new challenge when the polio programme detected an outbreak of circulating vaccine-derived polio type 2, a type of polio that emerges in places with low immunity. Dr. De Sousa again found herself at the forefront of the action, starting by supporting the Government to respond with vaccination campaigns.
One of her key tasks since has been recruiting new immunization health professionals, who can help reach the children missed by routine immunization and polio campaigns. She explains, “my goal is to train my colleagues so that we can work together to reach the vast number of Angolan children missing out on lifesaving vaccines.”
In July 2020, Angola held its first polio campaign after a pause on vaccination activities in the early months of the COVID-19 pandemic. More than 1.2 million children were reached by over 4000 vaccinators.
Gender and leadership
Dr. De Sousa explains that being a woman leader in Angola isn’t easy. “It requires a lot of time, dedication and a balance with domestic, family, and social life, which has not been easy to manage. However, with the help of God and my family – especially my husband – I am managing to carry out my work.”
“It has all been worth it for the results I’ve helped to achieve, and even though we have some way to go in relation to vaccination coverage, I’m grateful for the opportunity to ensure the health of our children and serve my country.”
In Angola, at the provincial and municipal level, there are very few women compared to men. However, in public health programmes at the national level, women outnumber men. Dr. De Sousa says that, “In general, I think there should be more women leading and administering vaccination programmes”.
In 2021, the polio programme is aiming to implement more outbreak response vaccination rounds to reach children with low immunity to the poliovirus. Driven by her passion and sense of duty, Dr. De Sousa will continue to be on the frontlines of this effort.
In 2018, Jawahir Habib, a Programme Officer in UNICEF’s Polio Outbreak Team based in Geneva, received a letter. It was from a Pakistani woman she had met while working in the Quetta block – one of the most high-risk polio areas of Pakistan. The letter read:
“I have four daughters, and my daughters are in school because of the polio programme. I can afford to teach my girls which my husband opposed. Now they too can get education and live an independent life. I will make sure every child is covered and this is my mission.”
Words like these inspired Jawahir and set her on a path to a ten year career in polio eradication. She recalls her first day at work, “That day was very interesting – I was chased by dogs in the Kharoatabad area of Quetta. Although I managed to save myself, I spent the whole day crying and realizing that polio workers face this type of adversity day to day. I knew that I must become a part of this and ten years later, I am still working to eradicate polio”.
Jawahir has over ten years’ experience in polio eradication. Despite the challenges, she has stayed motivated throughout.
The more Jawahir became involved in the polio programme, the more she witnessed women facing social challenges. At the time, suboptimal campaigns in the polio reservoirs was one of the major hurdles faced by the programme and the number of missed children in Quetta block remained very high. More than 70% of frontline workers were male or non-locals, resulting in limited access to households.
It was then that the Pakistan programme began looking at success stories from other parts of the world, including Nigeria, where Volunteer Community Mobilizers (VCMs) were making significant strides in eradicating polio. The need to build a network of local female health workers who were trusted and could gain access became more and more clear. Balochistan, where Jawahir is originally from, is one of the most remote and conflict-ridden areas of Pakistan and strict conservative religious and cultural norms, tribal conflicts and insecurity would prove very challenging.
When Jawahir’s team started recruiting, training and deploying women frontline workers in Quetta block, she was told it was impossible. “I was told that there was no way we could manage a workforce comprising of women working in these areas”. As a team leader, Jawahir had to create an enabling environment for women to work, keep them motivated and ensure systems were in place for them to reach every child in the block. “At a personal level, I had to lead by example and show everyone that women could work in these difficult areas, face resistance and achieve what a man could – in this case, even more.”
Jawahir knew well the challenges of being a young woman in a male dominated society. Born in Kili Mengal Noshki, a remote village in Balochistan bordering Afghanistan, she faced a lot of challenges. Despite this, Jawahir got her bachelors degree, a postgraduate diploma in public health management and a masters degree in health communication from the University of Sydney.
While working on polio, she had to work twice as hard as men, facing threats, gender biases and intimidation. What kept her inspired and motivated was being a part of something much bigger which she believed could change the world.
During this time, Jawahir’s team managed to identify, train and deploy a workforce of 3500 Community Based Workers (CBV) where 85% of the frontline vaccinators were women. During the first few campaigns 700,000 children in the core reservoir area were registered and vaccinated and more than 150,000 children who had previously been missed during the campaigns were mapped and given oral polio vaccine. One of the notable success of female teams was seen in Chaman Tehsil, on the border with Afghanistan, where within four months, the number of chronic vaccine refusals went from 15,000 to 400 children. That was a huge success for Pakistan’s polio eradication goal.
Jawahir attributes the success to the brave women who have made a major contribution to their society. She sees the empowerment of woman in one of the most difficult parts of the world as GPEI’s legacy of social change now and for the future. “Imagine a workforce of thousands of women having access to every household – imagine the venues we have for routine immunization, for nutrition, health and even education”.
The COVID-19 pandemic has compounded a rise in polio cases in Pakistan in 2019 and 2020, and polio eradicators once more have their work cut out to bring down virus transmission and protect populations.
“I believe now it is the responsibility of each and every one of us in the polio programme, whether a polio worker in Chaman or an Officer in Geneva, to ensure that this disease is eradicated once and for all. We will carry on no matter the hurdles and obstacles placed on our road, and we will finish the race.”
Ms. Rina Dey has spent over 25 years working in health and development, including front-line efforts to eradicate polio in India and globally.
“Unless we work at the community level, we’re not getting the full story. Ensuring community participation is the only way to achieve social transformation and to ensure that all children get immunized,” she explains.
In her role as Director of Communications for the CORE Group Polio Project, Ms. Dey works tirelessly to bring community perspectives to decision-makers at the national and state levels. Ms. Dey also continues to share lessons and innovative strategies from her work in India with other parts of the world impacted by polio.
Regardless of the location, her message is the same, “We need to take the time to listen. All questions and concerns are valid when it comes to making decisions about the health of one’s family – each deserves to be heard, understood and acted upon – without this, we will not be successful in protecting children.”
India, once thought to be the most difficult place in the world to end polio, was declared wild polio-free on March 27, 2014. A large part of this huge success was the ability to work one-on-one with communities in high-risk areas.
Ms. Dey began working in polio as a front-line Health Information, Education and Communication Officer with UNICEF and WHO.
She remembers, “Early in my career, during a field visit to Meerut, Uttar Pradesh, I came with a vaccination team to a house for polio immunization. A man came to the door, armed with a sword, and shouted that he would kill his nine-month old daughter, if we tried to enter and give her polio drops. I took a step back and directed our team to leave the house. It shook me.”
After taking the time to listen to the man’s concerns, Ms. Dey learned that the man was receiving a lot of misinformation from friends as well as his workplace. Out of fear and misunderstanding, he made the most severe threat possible to try and keep the health workers away from his family – in his mind to protect them.
“After taking the time to really listen to him and his friends, we began talking. I assured him that no one would vaccinate his daughter without his permission.”
Health workers need the knowledge and skills to effectively deal with these types of situations and to ensure that communities are receiving accurate information to make choices about the health of their families.
“The key is to address their questions and to build trust. By the following day, he welcomed the vaccination of his daughter and even went on to become an influential member of the community helping to address the concerns of other families.”
Ms. Dey decided to re-shape the way frontline health workers were trained.
“We needed to equip the health worker and vaccination teams with accurate knowledge and enhanced communication skills to understand and address the concerns of the families. There were many myths and misunderstandings to dispel, so I have put a lot of thinking into developing simple and user-friendly materials and methods which are local and participatory.”
“Investing in building capacities of frontline workers works! If they are not technically sound, they won’t be able to answer people’s queries.”
The Moradabad district in Uttar Pradesh was once an epicenter for polio outbreaks globally. Today, a monument to the district’s success stands tall above the bustling traffic of Moradabad City.
The monument is comprised of a large mother and child sculpture surrounded by the slogan “Two drops of life“. A polio vaccine vial sits on a base with four panels describing the partnership, strategies and journey to a polio-free India.
“No one thought it could be done when we started, but people from Uttar Pradesh, Delhi and West Bengal supported the polio eradication cause with high spirit and the job was done peacefully. A sense of great pride remains in Moradabad, and the whole of India.”
“When communities are heard and feel a sense of pride in the effort, sustained change is possible. But the flip side is also true.”
Ms. Dey remembers how children would come running with excitement, waving and cheering to interact with her team.
“When we were out on visits, the children would run to greet us. They wanted to know who we were, why we were in their neighbourhood and what we were doing. We would talk with them – we knew their names and what they were studying.”
“However, after some time, I realized that the children stopped coming, and some even began hiding from us. This was heartbreaking.”
Communities were being told that the vaccines could cause infertility, and parents were telling their children to run away from immunization teams. Dey took these insights to heart. She pushed her team, government officials and partners to think differently.
“I never thought of quitting. I want to see a polio-free world in my lifetime. I love children. I am working so that they can have a healthy life.”
She decided to develop strategies that would ramp up the involvement of influential members of the community, parents, schools, local government and families to ensure that accurate information was accessible to community members.
“We worked hard, and the scenario changed. Parents deserve to have accurate information so that they can make informed decisions about their children’s health. Many of those we engaged in this project are still advocates for polio eradication and immunization today.”
Women’s contributions cannot be overlooked
The Moradabad monument celebrating polio eradication in India.
“At ground level, we have lots of female health workers. In many countries a majority of frontline health workers and vaccinators are women, but at the higher levels, we find that the majority of leadership positions are held by men.”
“Women can often be sidelined in meetings. Things have improved, but we have more work to do. When women are in leadership positions, you find that other women are promoted and women’s voices from community level are more often heard.”
Ms. Dey recalls her own experience, “Once during a discussion with community leaders, I was not allowed inside one of the prestigious religious institutions. Even as a senior member of the team, I was made to wait outside for hours, while my male colleagues were permitted to speak with the officials inside.”
When asked what advice she would give to women beginning their careers in public health, Ms. Dey says, “Be a good listener. You must visit communities, spend time with them and build strategies for your work that are grounded in the realities of the people you are aiming to reach. You must make communications simple and always put appropriate ingredients into your approaches.”
“The health of our children and families is a very personal and foundational aspect of human life. Ultimately to increase vaccine acceptance, we have to relate to people on a human level first before launching into the science.”
“We’re always ready to give answers, but we also have to listen – at every level,” says Ms. Dey. “We must move away from being instructive and take the time to see people’s concerns as valid and to help people understand the science behind what we’re asking them to do.”
Dr Elaha, at 22 years old, is a medical graduate and a District Polio Officer. She’s also helping fight the COVID-19 pandemic in Afghanistan.
“COVID-19 has affected both our work life and personal life. When I joined the polio team, I had plans to take initiative and look for innovative ways to fight polio, however, with the COVID-19 pandemic all my plans were challenged,” she says. “Campaigns were postponed and the number of cases were on the rise.”
The temporary pause in polio vaccination campaigns, necessary to keep health workers and communities safe during the early months of the pandemic, led to a widened immunity gap in both Afghanistan and Pakistan, the only two countries that still harbour wild poliovirus. Now, polio teams are urgently working to close the gap while continuing their support to Afghanistan’s COVID-19 response. To ensure their safety, all polio personnel have been trained to take precautionary measures against COVID-19, including wearing masks correctly and regular handwashing.
Dr Elaha doesn’t underestimate the danger of her work to fight COVID-19. She explains, “I start my day at 8am by visiting private and public clinics, pharmacies, traditional healers at their homes. Of course, I am worried about myself and my family getting COVID-19. My mother is elderly, and COVID-19 can be dangerous for her.”
“However, I am committed to serve my people and go out in the field to help save others’ lives. It is not easy. My family understand that I am a medical doctor, so no matter what virus is there, I have to do my job as a doctor.”
Through her work, Dr Elaha has come up against rumours and misinformation. A major part of both ending polio and fighting COVID-19 is working to inform and build trust with communities about diseases and how they can be prevented.
Elaha says, “A lot of people thought that COVID-19 was a disease of nonbelievers. At first, when I used to go to clinics, because of my medical degree, they respectfully listened to me. However, when I talked about COVID-19 and washing hands and other preventative methods, they would tell me that this disease was for nonbelievers.”
“Unfortunately, a lot of people got sick and many also lost their lives. People have started to believe the pandemic. They know that people can get sick and die of the disease.”
Although public awareness about the dangers of COVID-19 has improved, Dr Elaha believes there is still plenty to do to encourage communities to adopt disease prevention measures such as widespread mask wearing.
Until the pandemic is over, she is determined to work long hours to fight both polio and COVID-19. The polio workforce currently contributing to COVID-19 response includes almost 36,000 members of the Polio Surveillance Network, and over 47,000 polio frontline workers.
Meet Sue
Whether in Pakistan, Seattle or Somalia, Dr Sue Gerber, a Senior Program Officer at the Bill & Melinda Gates Foundation (BMGF), is working with partner organizations to support polio workers – those delivering vaccines, educating the public or conducting disease surveillance.
Dr Sue Gerber (Senior Program Officer, Bill & Melinda Gates Foundation)
“The more time you can spend getting your shoes dusty walking and working together in the field, the better you will understand the challenges,” she says.
On one trip to Borno State in Nigeria, Gerber spent a week with community vaccinators – all well-respected women who, despite the massive geographic region they had to cover, maintained good spirits throughout their long travels. Across her work, Gerber finds motivation by staying closely engaged with the needs of those on the frontlines of the polio eradication effort.
Starting Out
While she studied to be an epidemiologist in college, one of Gerber’s first global health experiences was in the Peace Corps in Liberia, working with an immunization programme combatting childhood communicable diseases. Here, Gerber coordinated with Rotary International to secure meal funding for health workers travelling long distances to vaccinate children, foreshadowing collaboration integral to the GPEI. While in the Peace Corps, she found mentorship with legendary smallpox eradicator Stan Foster, who not only helped inspire her to work on polio eradication but also pointed Gerber toward her next role at the U.S. Centers for Disease Control and Prevention (CDC).
Gerber began work at the CDC on sexually transmitted diseases, first in California, and then later in Botswana and other countries in Africa. While in Los Angeles, she relied on frontline workers to help inform counseling and testing sessions assisting women with STD testing access in low-income areas.
Gerber’s next move was to CDC’s Global Immunization Division (GID) to support polio eradication in East Africa and Nigeria. She returned to the U.S. to lead GID’s Africa team for diseases of eradication and elimination, later serving as Deputy Director of CDC’s Namibia country programme.
Committed to Polio
Working collaboratively to combat other infectious diseases around the globe paved the way for Gerber to dedicate her career to polio. First at the CDC and now at the Bill & Melinda Gates Foundation, Gerber’s role in polio eradication efforts has evolved, but her drive to support health workers at every turn has remained steadfast.
“My responsibilities change over time depending on need and circumstance,” says Gerber. Currently, she supports polio eradication in Pakistan, by working with the national Emergency Operation Center (EOC) to improve supplemental vaccination campaigns and routine immunization services, and support integration with other primary health care services.
Gerber also supports efforts in Somalia, partnering with a variety of international organizations to work directly with in-country teams strengthening surveillance. As a member of the global surveillance task team, she develops strategic plans, guidance, trainings and assessments, incorporating frontline worker input on best practices for accessing hard-to-reach and insecure areas.
Innovating During a Pandemic
The resilience of frontline workers in the face of crisis continues to be the backbone of combatting diseases. This is especially true for today’s polio programme amidst the current global pandemic. While COVID-19 temporarily interrupted immunization delivery, Gerber remains optimistic about global health progress, adding that “during this pandemic, technology use has helped create innovative solutions to key problems.”
During the pandemic, polio programme assets have been instrumental in supporting COVID-19 response efforts. In almost every country with GPEI infrastructure and resources, polio staff have lent their expertise to conducting COVID-19 surveillance, combatting misinformation and sharing coordination mechanisms for pandemic response alongside programmatic activities.
The Role of Women
“Women have always been a critically important part of the programme, especially at the frontline,” says Gerber.
Across polio-affected countries, female vaccinators are crucial to building community trust and reaching all children, especially in communities where cultural norms prevent men from entering households. Despite this outsized importance to the programme, women are still heavily underrepresented in authority and management positions.
Ensuring that more women are at the table making decisions is a key part of Gerber’s drive. “Effective leaders lead from who they are,” Gerber says. By fostering strong working relationships, mentoring younger women and taking the time to listen to frontline workers, stakeholders and leaders, Gerber is able to channel her strengths and perspective as a woman into her role in eradicating polio.
Gerber adds, “I also think that representation matters. When women see women taking on a leadership role, they feel confident to lead and contribute in their own way.” In her own experience, seeing women mobilizing global resources, devising strategies or sparking catalytic action has provided an incredible source of inspiration.
What’s Next
Gerber is proud to be involved in eradicating polio – from working in the field to supporting new policies and approaches to bringing much-needed perspectives to the table – all while ensuring that “frontline workers are knowledgeable, prepared and protected.” Gerber is also working with Johns Hopkins University and their consortium partners on an academic course disseminating lessons learned from polio eradication efforts.
Her advice for the next generation of public health workers wanting to follow in her footsteps? “If you’re thinking about going into public or community health, please know you can make a difference.
“I chose to continue to do public health awareness during the COVID-19 pandemic. I wanted to help save people’s lives and continue to serve my people,” says Farida, a polio worker and volunteer for the COVID-19 response.
Seven months since the first COVID-19 case was reported in Afghanistan, female polio programme frontline workers continue to support outbreak response. Often, they put concerns for their health to one side as they work in areas with many COVID-19 cases. Sometimes, their work brings them into conflict with the social norms of their community and society.
Farida has been working with the polio programme since 2010. Starting as a volunteer, she has moved up the ranks to become a district polio officer.
During the pandemic, Farida has taken on extra duties to identify suspected COVID-19 cases, share accurate information and trace individuals returning from abroad to ensure they are isolating.
On a typical day she heads out to speak to small groups of women about hygiene, breastfeeding, nutrition and measures to prevent COVID-19. She is the focal point for communicable diseases within her clinic, and so must also keep all her colleagues up to date on the latest information about COVID-19, alongside reinforcing knowledge about polio and the importance of vaccination.
Farida’s work is often emotionally challenging. “Luckily, I still have not contracted COVID-19,” she says.
“I reported seven people as I suspected that they had COVID-19, unfortunately six of them died and one of them survived and is healthy now.”
Ever since the first case of COVID-19 was reported in Afghanistan, the Polio Eradication Initiative (PEI) programme has been supporting the government response.
Since March 2020, nearly 36,000 members of the Polio Surveillance Network, almost 44,000 polio frontline workers, about 95,000 health providers and about 5,000 government and NGO staff have been trained on COVID-19 surveillance. Over 178,000 community and religious influencers have been trained to deliver outreach messages, and almost 7,000 coordination meetings have been held.
About 10,000 COVID-19 and polio surveillance visits have been made to health facilities, and more than 2,500 medical facilities have been surveyed for COVID-19 preparedness. Thanks to the efforts of the polio team, over 46,000 cases of COVID-19 have been detected, of which more than 8,000 have been confirmed.
Farida shares with her colleagues a sense of duty to her fellow citizens. She says, “I go out hoping that my work might save lives. If I stay home, who will give the information to people that I do?”
After the World Health Assembly passed a resolution to eradicate polio worldwide in 1988, the Global Certification Commission led the way in establishing a formal certification process, asking each of the six WHO regions to set up a Regional Certification Commission. Then in 1996, the WHO Regional Director for Africa created the Africa Regional Certification Commission (ARCC) for Polio Eradication: a 16-person independent body tasked with overseeing this process, and later on containment activities in the African region.
Professor Rose Leke, an infectious disease specialist, has been the chairperson of the ARCC since it was set up in 1998. A trailblazer for women in global health, Leke has fought throughout her career to improve women’s representation in science and global health leadership. In 2018, she was one of nine women honored with a Heroine of Health award, recognizing her outstanding contribution to health care.
Stopping the ‘havoc’ of polio in Africa
Professors Leke explains her motivation to join the polio eradication cause, “When I was invited to be part of the ARCC in 1998, I was not involved in any polio-related work. But I could see the havoc that polio was reaping on the continent. I had a nephew who was paralyzed from polio and suffered brain damage, and another relative who contracted polio and continues to inspire me. Back then, you saw so many paralyzed young people on the streets. You don’t see that today.”
Ridding the African continent of wild poliovirus is a huge achievement, many years in the making. Nigeria, the last bastion of the wild virus, proved a particularly tough setting in which to vaccinate every child and ensure that no trace of the virus remained.
Professor Leke reflects, “It’s been such a long road. When Nigeria didn’t report any cases of wild polio for two years between 2014 to 2016, we were apprehensive but satisfied. We were so close to eradication as a region, everything was going so well, and then wild polio was reported again in Nigeria in August 2016, and certification had to go on the back burner.”
“The Nigerian response to their outbreaks has been extraordinary. Everyone is committed and highly involved. In Sokoto and Kano states, where I was recently for a field verification visit, and in all other states, everyone – from government officials, traditional leaders, health staff and field teams, community health workers and informants, polio survivors to traditional birth attendants – was heavily engaged in the response. The innovative technologies that have emerged have similarly been incredible. The Nigerian Emergency Operations Centre is a well-coordinated structure that is behind Nigeria’s success. Other disease programs in Africa are learning from this.”
Professor Leke never lost her drive to end polio, even during difficult years and despite the tough choices her role sometimes presented.
“When we started, we were aiming for wild polio to be eradicated by 2000; the thought of this success really kept me motivated and still does. At times it has been a huge sacrifice; as Temporary Advisers, ARCC members are not paid, and I’ve sometimes given up consultancies to do this work. My husband, children and grandchildren will tell you, there was a huge amount of traveling and many meetings. But I don’t regret the time spent for a moment on such a cause.”
“When Dr Moeti was appointed as WHO Africa Regional Director in 2011, this was further motivation to continue: I wanted to support a fellow woman. In the beginning, I was the only female in the Global Certification Commission. The commission has addressed this imbalance and we are now two females out of the six members. We need more women in senior positions on the African continent.”
Fighting for gender equality in global health and science
In 2011, Professor Leke won the Kwame Nkrumah Award for the best female scientist in Central Africa for her research on malaria. As part of her acceptance of the award, she took a pledge “to help promote the participation of women in science in Cameroon.”
Within a year, she had helped set up HIGHER Women, a mentoring programme for senior female scientists to deliver hard and soft skills training to their early career counterparts. To support the programme, Professor Leke contributed some of her own funds.
Professor Leke says, “As a woman I encountered blocks on the way during my career – at times men asked me to leave the laboratory space I was working in.”
“Science can be a pyramid – there are many early women researchers, but far fewer at the top of the field. Research and academia have a ‘publish or perish’ culture which disadvantages women who have responsibilities outside of the lab – such as raising a family.”
Professor Leke has continually used her position to promote women in science and global health, even sharing her favorite motivational track about women’s empowerment.
Whilst great progress towards gender balance has been made since she started her career, Professor Leke is firm in noting that there is more to do. In the African regional polio programme, women still lead only a small number of national committees.
Professor Leke is proud of the public health legacy that the polio eradication programme will leave in the African region. She says, “The polio response has brought many skilled technicians into Africa’s health systems. The GPEI paved the way for working closely with traditional healers and community leaders and has really helped to strengthen the systems that report on other diseases. The polio laboratory network is being used for other diseases, giving capacity in the region for doing all sorts of other diagnostics. You’ll find the one person in the health center who was there for polio is reporting on many other diseases.”
“After we declare Africa as free of the wild poliovirus, the ARCC will work with countries to ensure they keep up good quality surveillance, and improve routine immunization, keeping population immunity as high as possible. We will also continue to guide countries in continuing to monitor population immunity to prevent importations of wild poliovirus from outside the African region, while ensuring that the threat of circulating vaccine derived polio viruses (cVDPVs) is addressed.”
“Our work continues until all forms of polio have been eradicated globally.”