The stories below highlight some ways in which women are breaking barriers, driving change and inching us closer to a polio-free world wherever they take charge – from doorsteps to laboratories to decision-making tables.
Driving regional solidarity for polio eradication
Dr Hanan Balkhy, WHO Regional Director for the Eastern Mediterranean
Dr Hanan Balkhy made history in February 2024 when she became the first woman to take up the post of WHO Regional Director for the Eastern Mediterranean. With unwavering determination, she embarked on her new role with a clear vision: to eradicate polio during her tenure.
In her nomination speech, she shared her inspiration, drawn from success stories of joint efforts across the WHO Eastern Mediterranean Region. Dr Balkhy fervently believes in the need for collective action to overcome the obstacles in the path to polio eradication.
Dr Balkhy will convene the Regional Subcommittee for Polio Eradication and Outbreaks. To champion the Region’s work to consign polio to history, she will support the regional polio eradication programme, remove obstacles and work closely with global and regional decision-making bodies.
She calls upon all stakeholders to unite with resolute determination until polio becomes nothing more than a distant memory.
Blazing a trail with the Regional Subcommittee
Her Excellency Dr Hanan Mohamed Al Kuwari, Minister of Public Health, Qatar
An inspiration to women globally, Qatari Minister of Public Health H.E. Dr Hanan Mohamed Al Kuwari has been harnessing decision-makers’ power to galvanize action for polio eradication.
As Co-Chair of the Regional Subcommittee for Polio Eradication and Outbreaks since 2022, she has created a strong sense of solidarity among Member States of the Region and partners, reminding them of the urgent need to prioritize polio eradication. Using every possible chance to highlight the challenges faced by countries with wild or variant poliovirus cases, she has mobilized action to reach vulnerable children with polio vaccines and other health services.
Dr Al Kuwari has used her platform and voice to reveal issues faced by polio eradicators in the Region and offer solutions. At the same time, she has raised the visibility of the trailblazing Regional Subcommittee’s goals and work.
Integration involves using polio tools, staff, expertise, and other resources to deliver important health interventions alongside polio vaccines – from measles vaccines and other essential immunizations to birth registration, counselling on breastfeeding, hand soap and more. It also includes incorporating polio vaccines into other planned health interventions when possible, delivering more services with fewer resources.
There is no one-size-fits-all approach to integration. From the remaining endemic countries to countries affected by variant poliovirus outbreaks, activities must be country-driven and adapted to fit the unique challenges and needs of different communities.
Humanitarian engagement in Afghanistan:
In Afghanistan, supplementary immunization activities are essential to vaccinating children. However, in the context of an unprecedented humanitarian crisis and extremely fragile health system, integrating polio efforts with other health services has helped the program reach even more children.
Endemic transmission of WPV1 in Afghanistan has been restricted to the east region. Remaining pockets of inaccessible, unvaccinated children amid a broader humanitarian crisis pose challenges to stopping the virus for good. Today, more than two-thirds of the country’s population is in serious need of food, clean water, functioning sanitation facilities, and basic health services.
Building upon a strategy that has been in place for several years, ongoing collaboration with humanitarian organizations has demonstrated the value of integrating polio efforts with other health needs in the country. In 2023, the program began engagement with ten humanitarian partners operatingin 12 high-risk provinces for polio across Afghanistan. Through these collaborations, the program and its partners have mapped and supported communities that lack basic health services, which has helped better identify and reach children still vulnerable to polio.
Between January and October 2023, more than 1 million polio vaccinations have been delivered through the engagement with humanitarian partners. Through this effort, it’s estimated that more than 30,000 children have been vaccinated who would have otherwise remained inaccessible to the polio program during its standard campaigns¹.
The Far-Reaching Integrated Delivery partnership in Somalia:
In Somalia, children are at high risk of encountering and spreading the poliovirus due to longstanding security challenges and a lack of health infrastructure, particularly in the south-central part of the country. As a result, the country has historically low routine immunization levels and faces the world’s longest-running outbreak of type 2 variant poliovirus.
To help address these challenges, in October 2022, the GPEI partnered with the World Food Program Innovation Hub, Save the Children, Acasus, and World Vision’s CORE group, amongst others, to launch the Far-Reaching Integrated Delivery (FARID) partnership. The partnership’s primary goal is to stop poliovirus transmission and reduce deaths from preventable diseases and malnutrition.
To do this, the polio program and its partners have established a series of health camps across 20 districts in the country that provide families with vaccinations for polio and other infectious diseases, maternal health services, nutrition screening and supplements, and primary health consultations². These camps are tailored to address each community’s specific needs and aim to re-establish sustainable health systems that will continue providing primary health services on a routine basis.
Between October 2022 and June 2023, FARID partners have visited 136 high-risk communities in Somalia, reaching almost 30,000 people; vaccinating more than 8,000 children, 6,000 of which had never received any kind of vaccine; and conducting over 10,000 maternal health and 4,000 nutrition consultations³.
Read more about the polio program’s latest integration efforts here.
Acknowledging that our common goal is to attain ‘Health for All by All’, which is a call for solidarity and action among all stakeholders;
Noting the progress achieved globally in eradicating poliovirus transmission since 1988;
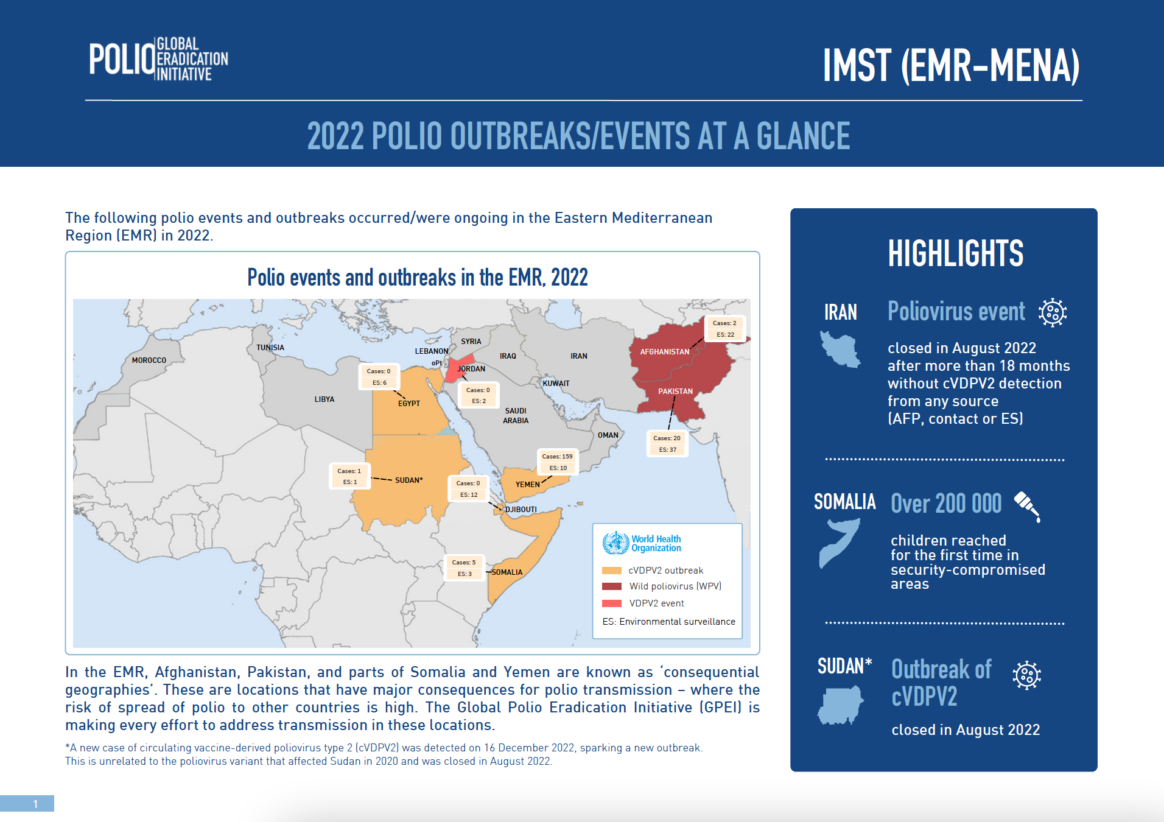
Noting with deep concern the challenges involved in stopping ongoing outbreaks of circulating vaccine-derived poliovirus type 2 (cVDPV2) in the Region, without full access to vaccinate all vulnerable children in the affected populations;
Observing with alarm the prolonged outbreak in Yemen and the persistent restrictions on implementing outbreak response vaccination in the country’s northern governorates, and further observing that the cVDPV2 outbreak which has been continuing since 2017 is the world’s longest ongoing such outbreak;
Recognizing the Global Polio Eradication Initiative’s efforts to target its resources in the most impactful way by identifying particular areas affected by polio, including Yemen’s northern governorates and south-central Somalia, as “consequential geographies” – two of seven subnational geographies globally which together accounted for 90% of all polio cases in 2022 and which are all affected by broader humanitarian emergencies;
Recognizing the high risk of expansion of the polio outbreaks within and from the two Regional consequential geographies due to their complex emergency settings, limited access to high-risk populations, weak immunization services, gaps in coverage of supplementary vaccination campaigns, and unmitigated spread of misinformation and disinformation in northern governorates of Yemen;
Recalling that the international spread of polio is a Public Health Emergency of International Concern under the International Health Regulations (2005);
Observing with alarm that 197 children have been paralyzed by cVDPV2 in Yemen’s northern governorates, representing almost one-third of all global cases of this strain in 2022, and that the international spread of poliovirus from Yemen to Djibouti, Egypt and Somalia has been confirmed;
Recognizing the best operational approach and experience to vaccinate all children, especially infants and young children, against polio, and achieve more than 90% coverage to stop an outbreak is through house-to-house delivery of vaccination; and if that is not possible, to implement an intensified fixed site vaccination with effective mobilization of families and young children to fixed sites near their homes;
Recognizing the continued threat to all children posed by vaccine-derived poliovirus and the importance of regional solidarity and support to deliver on the goals of the 2022-2026 Polio Eradication Strategy, which have been endorsed and supported by a wide range of committed donors, such as Rotary International and Member States of the Region, in particular the UAE through the sustained commitment of His Highness Sheikh Mohamed bin Zayed Al Nahyan, President of the UAE;
We, the Member States of the Regional Subcommittee on Polio Eradication and Outbreaks for the Eastern Mediterranean:
DECLARE THAT:
The ongoing circulation of any strain of poliovirus in the Region is a Regional Public Health Emergency;
COMMIT TO:
Mobilizing all needed engagement and support by all political, community and civil society leaders and sectors at all levels to successfully end polio as a Regional Public Health Emergency;
Advocating with relevant community and subnational leaders to increase access and ensure full implementation of polio outbreak response in the most programmatically and epidemiologically impactful operational manner, ideally through house-to-house vaccination campaigns in all areas;
Focusing efforts on reaching remaining zero-dose children in the consequential geographies of the northern governorates of Yemen and south-central Somalia, working in the broader humanitarian emergency response context;
Helping to mobilize needed resources and highest-level international commitment to finalize and fully implement the Somalia Polio Eradication Action Plan 2023, in the context of competing health response priorities such as ongoing drought and the effects of the COVID-19 pandemic;
Helping to mobilize resources for the Global Polio Eradication Initiative partners to support the outbreak response in Yemen; and
Helping to strengthen coordination with other public health and humanitarian efforts in Somalia and Yemen, to ensure closer integration in particular with routine immunization and the delivery of essential health and nutrition services to children;
REQUEST THAT:
The international humanitarian and development communities scale up their support for providing essential services, including a robust vaccination response to the polio outbreaks in Somalia and Yemen using modalities that will deliver an acceptable level of coverage;
The authorities and polio eradication partners in Somalia accelerate high-quality and rigorous implementation of the Somalia Polio Eradication Action Plan 2023 to stop the longest-running outbreak in the country and prevent the further spread of cVDPV2 by the end of 2023;
10. The national authorities and the Regional Polio Eradication programme strengthen cross-border coordination across Somalia, Kenya, Ethiopia, Yemen and Djibouti, considering the documented importation of cVDPV2 from Somalia into Kenya and Ethiopia, and from Yemen into Djibouti, Egypt and Somalia, and the high risk of further instances of cVDPV2 crossing international borders;
11. Authorities in northern governorates of Yemen, all immunization partners and the humanitarian development community respond urgently to the unmitigated vaccine-related misinformation and disinformation that is being disseminated, which is risking the lives of thousands of children in Yemen and across the Region;
12. All authorities in northern governorates in Yemen facilitate the resumption of house-to-house vaccination campaigns in all areas to ensure the delivery of vaccines to the youngest and most vulnerable children, and in areas where house-to-house vaccination is not feasible, make all efforts to implement intensified fixed-site vaccination through a modality that also includes robust social mobilization and outreach to ensure high coverage; and
13. The Regional Director continue his strong leadership and efforts to support the cessation of polio outbreaks in Somalia and Yemen, including by advocating for all necessary financial and technical support, reviewing progress, implementing corrective actions as necessary, and regularly informing Member States of the aforementioned and of any eventual further action required, through the World Health Organization’s Executive Board, the World Health Assembly and the Regional Committee for the Eastern Mediterranean.
Women make up only 28% of the workforce in science, technology, engineering and math (STEM), and men vastly outnumber women majoring in most STEM fields in college globally. On March 2011, the Commission on the Status of Women adopted a report at its 55th session to promote women’s equal access to full employment and decent work. Two years later, on 20 December 2013, the UN General Assembly adopted a resolution in which it was noted that it is imperative for women and girls to be involved in STEM.
On the International Day of the Women and Girls in Science on 11 February 2023, Rosemary Mukui Nzunza, the head of the Expanded Programme on Immunization (EPI) at the Centre for Virus Research, the Kenya Medical Research Institute, shared her story of pursuing a career in science. She is currently in the final stages of working towards earning her PHD in Molecular Medicine.
Rosemary explains she would like girls and women to know there is enough room for everyone in science; and women should maintain healthy competition in science and go as far as they can. It also helps to look for mentors and people you can admire and follow so they inspire you to keep growing, she says.
“Research has earned this name as it means you need to go back and search over and over again,” Rosemary says. “Besides, there are no ceilings in science – girls and women can go as far as they want to.”
As a child, Rosemary Nzunza spent her free time pounding leaves, roots and tubers, using thick wooden sticks to create “medicine”. Her creativity, curiosity, and love for finding explanations for how things work made her want to teach science − or at least work in the world of science.
Rosemary never has a dull day at work. She currently serves as Senior Research Scientist and Head of Division of the Expanded Programme on Immunization (EPI) at the Centre for Virus Research at KEMRI. Her role entails monitoring quality assurance in laboratory work and biosafety and overseeing the work of the different units at KEMRI. She also represents the laboratory in key national committees in Kenya: the National Committee on Containment of Polioviruses (NTF), National Polio Certification Committee (NPCC), National Measles and Rubella Technical Advisory Committee (MTAG) and the National Polio Experts Committee (NPEC).
Rosemary joined the Kenya Medical Research Institute (KEMRI) Laboratory 23 years ago, starting her career as a research officer with the US Army Medical Research Directorate (USAMRD). In 2006, Rosemary earned her Master’s in Applied Microbiology. Back then, she was one of just two women at the unit who had postgraduate degrees under their belts. She reflects on how her male colleagues looked up to the two women as mentors, which made them feel really proud. But she notes that this also meant they were in charge of all laboratory procedures, laboratory quality, and the troubleshooting, which was quite challenging at the time.
Polio still exists
When Rosemary joined KEMRI, she was surprised to learn that the institution was tasked with supporting polio eradication. She had thought polio had been wiped out from the world a long time ago.
Presently, Rosemary and her team at the KEMRI Laboratory work meticulously on testing samples of measles, polio and rubella. They know their work is integral to saving children from the harsh effects of preventable diseases, such as polio. Their work on polio is two-pronged: they have been testing samples for acute flaccid paralysis (AFP) since 2000 and environmental surveillance (ES) since 2013. AFP is defined by the acute onset of weakness or paralysis with reduced muscle tone in children. There are many infectious and non-infectious causes of AFP. Polio, caused by wild poliovirus (the naturally circulating strain) is one cause of AFP, and so early detection of AFP is critical in containing a potential outbreak. Respiratory and stool samples are optimal for enterovirus detection. Environmental surveillance complements AFP surveillance. It entails collecting and testing wastewater samples and can help in the early detection of and response to polioviruses. By identifying polioviruses swiftly, countries can stop their spread.
At times, the 17-member team receives an overwhelming number of samples at once from countries in the Region facing polio outbreaks. This presents a challenge, as it might mean the team needs more supplies for testing and needs to work longer hours to deliver timely results.
Once they have tested samples, they interpret results for each and send them back to the country to guide further and swift action. By 3 pm Eastern African Time every Friday, the KEMRI team works to send summaries of test results on measles, polio and rubella to the national surveillance office within Kenya’s Ministry of Health and other partners. These include the WHO Regional Office for Africa (AFRO); WHO Eastern Mediterranean Regional Office (EMRO); WHO headquarters; and the US Centers for Disease Control and Prevention (CDC).
Management during COVID-19 was a challenge
One of the most difficult times Rosemary has faced in her career was the response to the COVID-19 pandemic. During that period, she felt like health workers were carrying the weight of the entire world. In Kenya, her team was tasked with supporting the government in conducting COVID-19 tests. At the time, everything seemed so uncertain. Personal protective equipment (PPE) kits looked frightening, people all over the world were dying of COVID-19, and procedures and test kits still needed validation. She remembers thinking to herself, “Someone has to do this. And it’s us, here, now.”
Agnes Chepkurui, a lab technologist, preparing samples to determine what kind of poliovirus is present in the sample. Photo credit: WHO/L. Dore
Similar to the situation health workers around the world faced, her team was also afraid of being infected with COVID-19, especially before vaccines were available. Rosemary recalls the team staying at work for long, tiring stretches, partially to avoid contact with their families, out of fear of inadvertently putting them at any risk of being infected with COVID-19. Teammates would huddle together and discuss their after-work protocol at home: slip in through the back door, disinfect clothes, clean up rigorously, take a shower, avoid all contact with loved ones, and set off on the same routine the next day before anyone woke up.
She split the team into two shifts to manage the immense workload. The aim was to prevent the team from burning out and ensuring their new work on COVID-19 didn’t slow down the other, crucial support to disease elimination that still needed to be carried out. Looking back now, Rosemary credits the support she and her team received from the management at KEMRI, colleagues, partners, friends and family with helping them stay focused and rise to the unprecedented challenges of that time.
She also attributes the success of the KEMRI EPI Division Laboratories to support from institutions across the world, including the Global Polio Eradication Initiative (GPEI) partners. She says she has always been impressed with the incredible support from WHO and the rest of the GPEI partnership, where diverse agencies come together to tackle one goal.
More mentors needed for girls to join and grow in science
The young lady who stepped foot out of her village in Machakos county – in Kenya – for the first time when she left for Eldoret to earn her Bachelor’s in Science Education has come a long way. She is keen to see other girls and women take their place at the forefront of science – but only if they have a passion for this field, she adds. Breaking into a laugh, she says there’s a lot to read and keep up with every single day. After all, science is about changing the world.
On 21 March, the Federal Government of Somalia, World Health Organization (WHO) and members of the Global Polio Eradication Initiative (GPEI) recommitted to stopping the ongoing outbreak of circulating poliovirus type 2 (cVDPV2) in Somalia at a three-day meeting convened in Nairobi, Kenya. High-level delegates at the meeting included HE Fawziya Abikar Nur, Federal Minister of Health and Human Services, Dr Mamunur Rahman Malik, WHO Representative to Somalia and Head of Mission, alongside senior representation from the Bill & Melinda Gates Foundation (BMGF), the Centers for Disease Control and Prevention (CDC), Rotary International, Save the Children, the United Nations Children’s Fund (UNICEF), and other UN agencies and partners.
Together, the Government, GPEI partners, which include WHO, UNICEF, the BMGF, CDC, Rotary International, GAVI, the Vaccine Alliance, and other key partners endorsed the Somalia Polio Eradication Action Plan 2022 to reaffirm their commitment.
The Somalia Polio Eradication Action Plan 2022 outlines a four-point call to action to stop the spread of the current outbreak, which is one of the longest lasting cVDPV2 outbreaks to be reported so far. The robust plan aims to direct partners’ efforts and resources towards boosting population immunity, making concerted efforts to reach high-risk populations — including inaccessible and nomadic communities and internally displaced persons — to strengthen their immunity, enhancing the search for poliovirus circulation, and strengthening coordination among all stakeholders. Some of the strategies that will be deployed include intensifying efforts to offer 5 opportunities for vaccination against polio in 2022, providing routine childhood immunization in high-risk locations, where children have missed out on vaccinations, and strengthening community engagement. Given how easy it is for the cVDPV2 virus to spill over international borders, the emergency plan also advocates for stronger cross-border coordination among the polio eradication programmes in Somalia, Kenya, Ethiopia and Djibouti.
“In the midst of the ongoing drought, and while recovering from the effects of the COVID-19 pandemic, our stakeholders must not forget how important it is to contain the ongoing poliovirus outbreak so that it does not spread any further and does not affect any more children’s lives,” said HE Fawziya Abikar Nur, Federal Minister of Health and Human Services. “On this occasion, I would like to extend my sincere gratitude to all our partners, and donors, for the immense efforts they have put into shielding millions of Somali children from polio over the years.”
“Since its inception 25 years ago, Somalia’s polio eradication programme has made progress, including by stopping outbreaks of wild poliovirus and, recently, one of circulating poliovirus type 3 in 2021. The programme has established a vast network of polio workforce and assets and we can do more not only to stop the current outbreak but to achieve broader health system goals through integration and effective use of our human and operational resources. Since 2018, Somalia has conducted several supplementary immunization campaigns. Despite these efforts, pockets of unvaccinated children remain, due to insecurity and limited access to health services,” said Dr Mamunur Rahman Malik, WHO Representative to Somalia.
The Somalia Polio Eradication Action Plan, which will be implemented in 2022, complements one of the goals outlined in the GPEI ‘Polio Eradication Strategy 2022–2026: Delivering on a Promise’, to stop cVDPV transmission and prevent outbreaks in non-endemic countries. It is also in line with Somalia’s national goals and UN Sustainable Development Goals (SDGs).
Fahima Ahmed Hassan is a 25-year-old community mobilizer who goes the extra mile to ensure parents of children under the age of five are informed of Somalia’s polio vaccination campaigns and are ready for their children to be vaccinated.
Fahima and the other mobilisers are from the local community and they lay the groundwork for vaccinators ahead of campaigns. They work tirelessly to reach every house, speaking to families to help them understand, trust, and accept the vaccine.
On a mid-October morning, children and their families are waiting anxiously. They have been informed, by Fahima and through loudspeaker announcements, that a team of vaccinators will be visiting their community.
Amid the COVID-19 pandemic, some people are concerned and worried about taking their children for vaccinations. They fear they might contract the virus or expose their children to it. Together with her team, Fahima takes every precaution to keep herself and the community she serves protected.
She explains that it is critical to show the community that vaccination can go ahead while maintaining physical distancing, wearing protective masks and using hand sanitizer.
Some people do not need to be convinced about the benefits of immunization. Asha Osman Yarow is one of them. She is patiently waiting for her son to be vaccinated.
“I decided to vaccinate my children because their health is important to me,” Asha says, holding her young son. “Vaccines protect children against diseases, like polio, measles and others.”
“Praise be to Allah that these services come to us,” chimes in Sahro Mohamed Haile. “I encourage all mothers to take care of their children, vaccinate them and keep records of their vaccination status. Me, I’m here today with my grandson,” she adds with a smile.
Others in the community are more reluctant to accept vaccines. “At first, I refused to vaccinate my children. I heard people say that the vaccines were no good and that they were made by non-Muslims. I was scared,” explains 30-year-old Wardo. “After speaking to the community mobilizers, I realized that the vaccines are good for my children’s health – and I changed my mind.”
“I understand where they are coming from, and I do my best to give them information and convince them that vaccinations are beneficial,” says Fahima. “Illiteracy, lack of education and myths make people reject the vaccines.”
Together with the other community mobilizers, Fahima engages elders, religious leaders and community influencers as well as urging parents until the very last minute to come forward.
“I’ve vaccinated all of my children and I was one of the first people in my community to support vaccines,” says Isha Hassan Saney, a fellow community mobilizer. She believes showing a good example helps to convince others in the community to vaccinate their children.
“I am motivated to serve the community, especially the mothers and children, because they need to be taken care of,” Fahima says. “There is no better reward than seeing them healthy.”
COVID-19 shows why vaccines are so important
Despite COVID-19, and the enhanced risk of infecting her husband and her extended family members when she comes home, Fahima continues to show up for work and doesn’t let fear take over.
The COVID-19 pandemic has revealed what is at stake when communities do not have the protective shield of immunization against an infectious disease. When vaccines are available, they are the most effective tool to prevent dangerous disease outbreaks.
Staying informed about their benefits and understanding the risks of not getting vaccinated has never been so important. Fahima and the other community mobilizers play an instrumental role in this.
During the recent polio immunization campaign, 8 951 vaccinators went door to door and 3 390 community mobilizers, including Fahima and her team, sensitized communities. The two-part campaign, organized by the Federal Ministry of Health, UNICEF and WHO, reached more than a million children under the age of five in south and central regions of Somalia.
From 30 August to 3 September, Somalia conducted an integrated measles and polio campaign in the Banadir region – the first immunization campaign held since the COVID-19 pandemic reached Somalia. Over the last seven months, health workers have been fully engaged in fighting the pandemic. This campaign, conducted whilst observing safety measures to prevent spread of COVID-19, was a chance to get back on track to protect children who have missed out on vital immunizations.
Ismail Taxta/Ildoog/WHO Somalia
The campaign was conducted by Somalia’s Federal Ministry of Health, with technical support from WHO and UNICEF, and financial support from the Global Polio Eradication Initiative and Gavi, the Vaccine Alliance. The campaign had initially been scheduled to take place in 2019 as part of a nationwide effort, but was postponed due to technical challenges.
Ahead of the campaign, vaccines were procured and stored in optimum cool conditions. Microplans and maps were updated to help vaccinators reach all children at health facilities and fixed outreach sites. Building population immunity to polio and measles is extremely important in Somalia: Since the start of the year, 744 children in Banadir have contracted measles, accounting for half of the cases nationwide. Two forms of polioviruses, in circulation in Somalia since the end of 2017, have caused paralysis in 19 children across the country.
As part of the planning, 602 teams of health workers were given protective face masks and gloves, and were trained rigorously to keep themselves and their families safe from COVID-19. Every morning, they were checked to see if they had COVID-19 symptoms. Precautionary measures taken during the campaign included washing hands regularly, wearing face masks and ensuring physical distancing.
On the first day of the campaign, health teams set up fixed outreach vaccination sites and health facilities in different locations in Banadir. The aim was to reach as many children as possible: those living in urban and rural locations, those with nomadic lifestyles, and those living in camps for internally displaced persons.
All children under five who visited facilities during the campaign received deworming tablets and vitamin A, in addition to measles and polio vaccines. The inclusion of other health interventions in polio campaigns is a safe and effective way to help parents give their children the best possible protection against childhood diseases. This is particularly crucial in the Somali context, where children have limited access to health facilities, and population immunity is chronically low.
Two hundred and twenty-four district field assistants supervised more than 3000 vaccinators to ensure vaccinations were administered correctly and COVID-19 safety measures were observed. The campaign was also monitored by staff from the Ministry of Health, UNICEF and WHO.
Women and men played an important role in the campaign as social mobilizers, sharing messages on the benefits of vaccinations and COVID-19 prevention measures. Additionally, community volunteers helped to manage crowds of caregivers who visited health facilities and vaccination sites, ensuring that physical distancing was observed.
At the end of the day, all waste products from the campaign, including syringes, sharps and empty vials, were disposed of safely. By delivering multiple health interventions at once, cost savings can be achieved, and environmental impact is reduced when compared to delivering interventions separately.
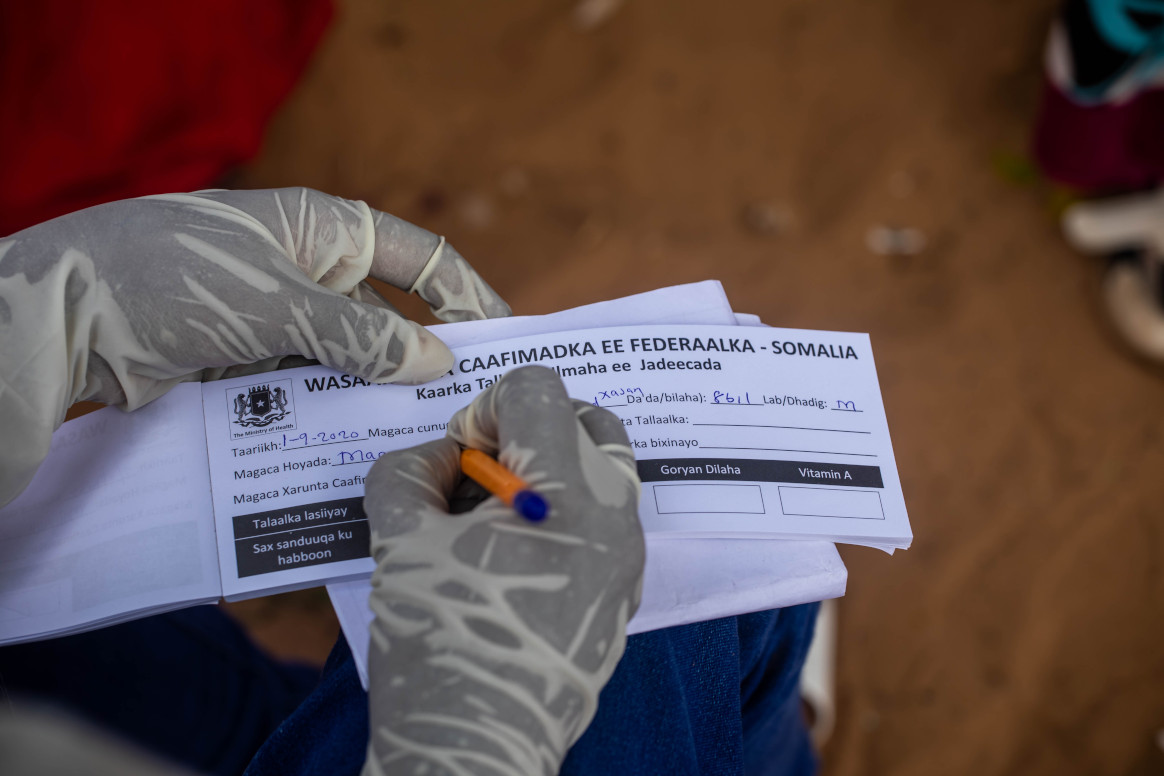
Vaccination teams provided caregivers with vaccination cards for children, so that monitors could keep track of children who did not receive measles and polio vaccines.
Around 408 000 children aged between six months and five years (92% of those targeted by the campaign) received vaccinations against measles and 459 000 children aged under five (93% of the target) were vaccinated against polio. Ninety-two percent of children also received vitamin A and deworming tablets. This campaign proved that delivering health interventions amid COVID-19 in Somalia is achievable – and paved the way for subsequent campaigns to fill immunity gaps.
For Somalis, COVID-19 is the most immediate crisis in a seemingly unending cycle of floods, food insecurity, conflict and outbreaks of vaccine-preventable diseases like measles, cholera and polio. Against this backdrop, the World Health Organization’s polio programme is working to steer the COVID response and, more broadly, maintain vaccine immunity levels and improve access to healthcare. It’s no easy feat.
Dr Mohamed Ali Kamil, the outgoing World Health Organization Polio Team Lead and COVID-19 incident manager for Somalia, is in awe of the commitment shown by health staff. He recently phoned a Polio Logistician diagnosed with COVID-19 who was experiencing symptoms, to insist he stop working remotely from his sickbed. Dr Kamil recalls, “He said, “No Sir, I will continue.”
Since the first COVID-19 case was diagnosed in Somalia on 16 March 2020, the polio programme has fought the pandemic from the ground up. Dr Kamil explains, “No other health programme has comparable expertise to serve the Somali population during COVID-19. During their time in the programme, members of the polio team have responded to many different disease outbreaks. This means they were well placed and well trained to respond to COVID-19.”
“The polio programme has spent years building staff capacity and systems to implement vaccination campaigns and detect the poliovirus in the community. In some ways, the team are the first and last line of defense.”
The response includes education, case identification, contact tracing, case management and data support. As of June, polio staff working as part of rapid response teams (RRTs) had reached 2.6 million people with messages about COVID-19 prevention. District Polio Officers within the RRTs have led the investigation of over 4500 people with suspected COVID-19 across the country. The country has set up three COVID-19 testing facilities and the polio structure established for the collection and shipment of stool samples from AFP cases has been used for the transportation of COVID-19 samples.
Throughout, polio personnel have continued their full-time work to end the circulating vaccine-derived poliovirus (cVDPV) outbreaks that have thus far paralyzed sixteen children since 2017.
The team are driven by a humanitarian commitment to the Somali population, who have suffered over 30 years of protracted conflict and insecurity. At least 5.2 million people are in need of humanitarian assistance, and secondary and tertiary healthcare is virtually non-existent outside of a few large cities. Health literacy is low, and populations are highly vulnerable to diseases like polio, measles, cholera and now COVID-19. In November 2019, widespread flooding brought further turmoil and danger to Somali families.
The team’s work is made more difficult by the emotional toll wrought by the pandemic. To date at least 143 health workers have been identified with COVID-19 infection. In April, Ibrahim Elmi Mohamed, a District Polio Officer who spent 19 years striving for a polio-free Somalia, died of a COVID-19-related illness. His death, one of many frontline staff around the world due to COVID-19, remind us of the risks they face every time they go to work.
Challenges lie ahead to defeat polio
Dr Kamil is clear that the polio programme will require ongoing funding and the support of authorities, partners and communities in order to maintain polio activities amidst the pandemic.
“To sustain the immunity gains we must implement a number of polio vaccination campaigns each year until the routine immunization programme can reach every Somali child with all polio vaccines. Somalia is extremely fragile and at high risk of becoming endemic for poliovirus if we do not maintain and support the polio infrastructure,” he says.
Since the cVDPV outbreaks were first detected in 2017, the programme has streamlined disease surveillance for cases of acute flaccid paralysis and other preventable diseases, including by introducing mobile technology to record details of suspected cases. For the first time, environmental disease surveillance was introduced. Over three years, frontline health workers have implemented more than 15 polio campaigns, including integrated campaigns with the measles programme.
Dr Kamil explains, “We still don’t know where the virus is coming from exactly. There are many inaccessible areas, where we cannot deliver vaccines or respond with immunization campaigns. We suspect that the virus is circulating among vulnerable children and communities living in these areas.”
Dr Kamil feels strongly that the polio programme has a duty to support other health interventions. He says, “COVID-19 shows what the frontline polio staff can achieve and the strength of surveillance and response systems.’’
Despite the challenges, Dr Kamil retains his belief that with ongoing funding and support, the cVDPV outbreaks in Somalia can be brought to a close. He reflects, “COVID-19 is a huge emergency in Somalia. Our staff are working flat out, and we expect to see many more cases, but at the same time we must continue to fight polio. The Somali community and the world deserve to be free of this disease.”
“We must reschedule our March polio vaccination campaign which was delayed because of the COVID 19 outbreak. We must do everything possible to keep health workers safe from COVID-19. It’s a hard situation, but we must not stop until we overcome both viruses.”
“The road to the mountain village was rough. It’s only 50 kilometres, but it took more than 3 hours,” says Dr Fatima Ismail, a disease surveillance officer working in Somaliland. “We were bouncing in the car.”
In early 2020, Dr Fatima’s team headed to a remote village near Djibouti to check on a small boy. The boy’s right arm and leg showed a kind of paralysis that sometimes indicates polio. “The village polio volunteer in this mountainous area, geographically inaccessible, found an acute flaccid paralysis (AFP) case,” Dr Fatima remembers.
When children show signs of this paralysis, it is critical to get stool samples to a laboratory to determine whether they have polio. Polio teams ride camels in the desert or donkeys in the mountains when they have to. They brave conflict to get samples to laboratories. In brutally hot climates, they plug mini-freezers into car dashboards to keep samples cool.
All over the world, polio surveillance systems that have been built up over decades track infection sources, evaluate symptoms and transport samples to the laboratory — despite distance, natural disasters, and sometimes war. Now, disease surveillance network — reaching into the most far-flung corners of the globe — is being tapped to address the COVID-19 pandemic.
“In Somalia, the polio programme pivoted its workforce of thousands of frontline staff to support the effort as the cases of COVID-19 spread. Rapid response teams — made up of disease surveillance officers, community health care workers and volunteers — were trained to educate people about the virus and to test suspected cases. By April 2020, the teams were deployed in the field,” said Dr Mamunur Malik, WHO Representative in Somalia.
“In Somalia’s remote villages, they know us as their polio teams, and once they see us, what comes to their minds is that we’re giving them information about polio,” says Mohamed*, a surveillance officer. “So we also give them information about COVID-19. Social mobilisers tell them about COVID-19 symptoms, how to prevent getting infected, physical distancing, cleaning their hands very well with running water and soap.”
The careful procedures that the teams learned for polio surveillance have been adapted for COVID-19, where the required sample is a naso-pharyngeal swab. “We’ve trained our surveillance people on the case definition and how to collect the samples correctly, from people that meet the definition of a suspected case of COVID-19,” says Dr Fatima. “It’s the same infrastructure. After, when we collect the samples from the patient, we send it to the laboratory in Hargeisa.” WHO has given the laboratory equipment and supplies to test samples for COVID-19.
“As with polio samples, the samples of COVID-19 have to be refrigerated, the ice packs should be VERY cold,” says Mohamed. Teams are used to monitoring the packs’ temperature, even in Somalia’s hot weather.
“The logistical challenges we face with AFP/polio surveillance are still the same. This is the rainy season and the roads tend to be terrible,” says Mohamed. “You can’t get to certain places you normally get to, because of the situation on the road. Most of our vehicles can’t make it through the mud.” In those situations, teams work with other United Nations agencies to arrange special humanitarian flights to ship samples.
Frontline staff put their own lives on the line. In April 2020, the polio team lost a colleague due to COVID-19-related infection. Ibrahim Elmi Mohamed, who joined WHO in 2001, was working as a district polio officer in Lower Shabelle. His tragic death, one of many frontline staff around the world due to COVID-19, reminds us of the risks they face every day they go to work.
“Despite overwhelming challenges, teams are committed to continuing their polio work in tandem with the COVID-19 response. It is critical that polio surveillance continues during the pandemic, as Somalia is also fighting outbreaks of vaccine-derived polio type 2 and 3. With polio vaccination campaigns temporarily paused, the teams must be able to track any resulting spread of poliovirus and get ready to respond as soon as it is safe to do so,” says Dr Malik.
“All of us are still doing polio surveillance at the same time as we do surveillance for COVID-19,” says Dr Fatima. “I used to hear from my colleagues that the polio surveillance system is the strongest disease surveillance system. Any polio surveillance team can work in the detection of COVID-19 cases because of the system’s structure, the capacity and experience of the teams.”
Mohamed agrees. “My surveillance coordinator said don’t leave the AFP surveillance behind, follow that normal routine, don’t forget it and leave it aside.’”
As Somalia grapples with the COVID-19 pandemic, its trained teams are working quickly to prevent the spread of both COVID-19 and polioviruses. “What gives me hope in the COVID-19 response is when I look behind and I see what we have done with the polio teams, the impact we’ve had on so many lives,” says Mohamed. “We face everything and we overcome it.”
Noora Awakar Mohammad was only sixteen years old when she started working as a volunteer for the Polio Programme in Somalia. Since then, she has lived through civil war and armed conflict in her country, which have left the health infrastructure in tatters. Recalling the days of war, Noora’s face tenses. “During the civil war years, on many occasions the polio campaign was stopped because of intense fighting. As soon as the fighting would stop, we would run to communities to vaccinate children,” she recalls.
During those days, it was mostly elderly women and mothers who trained as vaccinators. The adolescent Noora had to work hard to build community trust. “Often, I stayed with the community and vaccinated the children amidst war. The community trusted me even though I was a young health worker,” she remembers.
Noora still faces challenges in her fight against polio. Many areas in Somalia are unreachable because of the presence of non-state groups. These groups, who oppose vaccination, have been responsible for creating fear among parents by spreading misinformation. Noora has also encountered vaccine-hesitancy among parents because of inadequate health awareness. “I have seen fathers refusing to vaccinate their children on one hand, while mothers request us to vaccinate them on the other. Under such trying circumstances, we have to seek the help of religious leaders to convince the refusing fathers,” Noora explains.
Alongside polio vaccination, Noora works as a midwife. As part of her role, she educates pregnant women and young mothers about the benefits of vaccination. She also builds awareness of Acute Flaccid Paralysis (AFP) in the community, a key symptom of polio. “I share information about AFP with mothers and now I see more and more mothers bringing their children to health centers even with the slightest symptom of AFP,” Noora says.
Noora emphasizes that closing the current polio outbreak in her country remains tough given the climate of insecurity and inaccessibility, but she remains determined to carry on with her work.
Zainab Abdi Usman is a midwife in Madina district in Banadir state in central Somalia. For the last twenty years, she has volunteered for the polio eradication programme. A source of frustration for Zainab is the children missing out on vaccination in inaccessible areas. The barriers health workers face to access populations in desperate need of basic healthcare and community services are sometimes insurmountable.
“During the civil war, I used to carry the vaccine in a thermos kettle to keep it cold and I would hide it under my Abaya. If fighters got suspicious, they would not allow me to go into the communities to vaccinate the children. Today, many areas remain inaccessible,” Zainab says.
Whenever the access situation changes, the polio programme is amongst the first health initiatives to reach children. Zainab explains, “In a conflict situation, there is an immediate need to treat victims of the conflict. However, at the same time, it is important that we save our children from paralysis resulting from polio. Therefore, reaching out to children in insecure areas is very crucial in our fight against the disease.”
Feriha Abdur Rehman Yusuf is the young mother of a one-year old boy. She sees the fight against polio as personal and has been part of over 30 immunization campaigns in Somalia.
An incident from Feriha’s past stays with her years later. “One day, during a door-to-door campaign, I knocked at the door of a house. A man carrying a gun opened it. He yelled at me and started shooting in the air. I was shaken for days,” she remembers. Thankfully, the situation has changed in Feriha’s district since then.
Thanks to efforts to educate parents, the public is more aware of the long-term benefits of vaccination. However, Feriha still faces a few families who reject the polio vaccine during campaigns. She tries to convince parents using the examples of her own son, and her nephews and nieces. If families continue to be worried, she seeks help from religious leaders and community members.
Working during campaigns is not easy for Feriha now she has her son. Feriha says that her mother is the biggest supporter of her work and source of encouragement. “When I am in the field during the polio campaigns, my mother practically moves into my house and takes care of my child,” she says.
Feriha believes that despite the climate of insecurity and inaccessibility, things are improving in Somalia. “Health services are getting better than before. More and more children are getting vaccinated, so they have a better shot at life,” she says.
Abdullahi Mahamed Noor, hailing from Mogadishu in Somalia, wears multiple hats. By day, he is an experienced and dedicated polio programme zonal coordinator. By night, you can find him racing down the court as president of the Somali Basketball Federation.
Mahamed’s journey to end polio started in 1999, as a vaccinator in Adale District of Middle Shabelle in Southern Somalia. Since then, he has worked to combat multiple polio outbreaks in his country, including the current cVDPV outbreak.
Mahamed strongly believes that eradicating polio isn’t just about delivering the vaccine. To maintain high immunity levels, the programme must deliver a clear message about the safety and importance of the vaccine and help communities become better informed. To achieve this goal, Mahamed uses his sporting connections to combine basketball with innovative polio immunization messages, with the objective of increasing awareness throughout his community.
Last year, Mahamed took advantage of a Vaccination Week to deliver messages on polio eradication at several basketball games held in Mogadishu. “When people come to the stadium, they see messages on polio awareness and how important it is to vaccinate children to build their immunity against polio virus. They pass those messages to family and community members,” he explains.
From 1999 to 2010, a period during which Somalia suffered several polio outbreaks, the inaugural ceremonies of most of the major sports activities in Somalia would begin with statements encouraging people to vaccinate their children against polio.
Currently, Mahamed supports polio officers to develop comprehensive microplanning for immunization campaigns in Somalia. He emphasizes fostering trust between frontline workers and communities, since the polio workers in Somalia travel door to door to deliver vaccine. The basketball games that he organizes in his spare time help to increase acceptance of polio workers in the community.
“Part of my job is to convince the families who refuse to vaccinate their children. I quite often use my experience of being involved in basketball to educate them on benefits of polio vaccination and preventing disability related to poliovirus.”
Sportspeople are active in the fight to end polio the world over. Ade Adepitan, a British Paralympian, wheelchair basketball player and broadcaster, who is himself a polio survivor, is a strong advocate for polio eradication. In Pakistan, cricketers often promote polio eradication campaigns during the highly watched and well-attended matches.
In many parts of Somalia, poverty, conflict, internal displacement and weak health infrastructure often mean that vaccination levels remain relatively low. Amidst these trying circumstances, dedicated workers like Mahamed are playing a critical and innovative role in educating communities about polio and the absolute importance of vaccination to defeat the disease.
Environmental surveillance teams in Mogadishu access the underground closed drainage system to collect sewage waste water samples, which they package and send to the laboratory for testing. If poliovirus is identified in a sample, epidemiologists know that the disease is likely to be circulating amongst the community whose sewage drains into that part of the system. This process is called environmental surveillance and is one of the most important tools for the polio programme to help detect poliovirus.
Vaccinating every child and conducting disease surveillance to know where the poliovirus is circulating are key strategies to end the outbreak. Low immunization coverage has led to an outbreak of vaccine-derived poliovirus in Somalia. This can occur in places where not enough children have received their full vaccine doses.
The teams must follow best practice to collect samples, to ensure that any poliovirus present can be detected.
Click through this photo gallery to learn more about the sample collection process.
Mohamed Sharif Mohamed, Regional Polio Eradication Officer for Banadir, is responsible for organizing the collection of waste water samples at two sites in Mogadishu.
He explains, “Environmental surveillance was established in September 2017, when the outbreak of vaccine-derived poliovirus occurred.”
So far in 2019, 36 samples have been collected from four sites in the city as part of this important initiative.
First, Mohamed Sharif’s team put on face masks, aprons, and gloves. They are collecting untreated sewage waste water, so it’s crucial that they wear protective clothing to protect themselves from bacteria and viruses that they may encounter during their work.
Their next task is to detect the atmospheric temperature of the site, and record this on the lab request form.
The officers try to collect a high-quality sample from a pipe with running waste water. The sample must be free of contaminants, such as detergent liquids or rubbish, which could kill the virus before it is detected.
Mohamed Sharif explains that collecting a high-quality sample can be a challenge in Mogadishu, “The sewage system is old and poorly maintained. Often, rubbish is visible. Despite this, we try our best.”
Once the sample is collected, it is drained into a secure screw-cap container, which is sealed, cleaned with liquid bleach, and labelled with a unique ID code.
The ID code references this specific environmental collection site.
“Mogadishu is the first region in the country to establish environmental surveillance for polio,” Mohamed Sharif says. “The community, Ministry of Health, and the Mogadishu Municipality are aware of the hard work we are doing.”
The sample is put into a cool box for transportation to the WHO office. From there, it will be immediately flown to Kenya Medical Research Institute (KEMRI) in Nairobi, where there is a specialized poliovirus laboratory. This lab tests samples from countries across the Horn of Africa.
The sample should be kept at 4°c throughout the four-hour journey to the laboratory. This is known as the ‘reverse cold chain’ and prevents the virus deteriorating during transportation.
Packing a sample from Waberi District Site ready for transportation to the lab
Back at the office, the sample container is sealed in a plastic zip lock bag, and paperwork is completed. Then the sample is transported, surrounded by fresh icepacks, to Nairobi.
At the laboratory, a highly trained technician will analyse the sample for viruses.
Staff in Somalia follow up the results with the laboratory two weeks after the sample arrives at the lab.
Carrying a sample collected from Egyptian Hospital site
Mohamed Sharif explains what motivates him to continue this challenging work: “It is our hope that in future, when polio eradication is achieved, our names will be written in the offices of the Eastern Mediterranean region of the World Health Organization.”
“We will be part of the legacy of polio-free Somalia.”
Thanks to the unbending resolve and resilience of women health professionals as they go door-to-door across villages and mountains administering vaccine in some of the most marginalized or remote communities, women are truly the backbone of the polio programme at the ground-level. We asked a few of these women about their most daunting and heartening moments in polio, and how they worked through them.
Julia Kimutai—Community Strategy Coordinator Nairobi, Kenya
For Julia Kimutai, a 38-year-old community strategy coordinator in Kenya, educating the public about the importance of vaccines is a constant project. As a specialist in dense urban areas with high rise buildings, Julia knocks on a lot of doors and is often greeted with refusals.
“To convince some mothers is not easy,” she says. “It has never been a smooth ride.”
But where some might just see a campaign-time encounter with skeptical parents as a one-off, Julia sees a long-term project.
“Where we have difficulties is where we double down our efforts to build relationships. We even go back when there is no polio campaign to try to talk with parents, emphasize why vaccination is important and try to do a lot of health education,” she says.
As a woman and as a mother, Julia believes she is uniquely qualified as she can relate, understand and convey the importance of polio vaccines to the numerous apprehensive mothers she meets daily.
“I am a good listener, a good communicator and patient. These tools help me daily as Polio Eradicator and a mother.”
A district polio officer with over two decades of experience in Banadir, Somalia, for Asha Abdi Dini, refusals are always heartbreaking. “My worst moment was seeing a family who had three girls and a son. They vaccinated their daughters but refused to allow the boy to take the vaccine. The boy got the polio and the girls survived.”
But Asha takes pride in the challenges she has been able to overcome since joining the polio programme.
“My best moment is seeing the same children I once vaccinated all grown up and bring their own children for vaccinations. It gives me immense hope and happiness,” she says.
Bibi Sharifa—Health Communication Support Officer, Islamabad, Pakistan
A continent away, for 39-year-old Islamabad district health communication support officer, Bibi Sharifa, a big part of the job is demonstrating how women can do difficult work and stand firm in the face of adversity.
“People often think that women are incapable, but they really couldn’t be more wrong. The women on our programme are extraordinary – they are strong, gentle, dedicated, humble, passionate, disciplined and fierce at the same time,” she says. “They are driven by the love of their children and their community, and despite the challenges they face, people should realize that women are like grass, not like trees: where trees can be uprooted by floods, grass can face the brunt of flood easily.”
If you ask the women who work in Somalia’s polio programme why they do what they do, most will tell you they do this to help Somali children, to build a stronger future for Somalia, and to support their own families. Somalia is a complex country with many cultural and institutional challenges for women who work outside the home. Perhaps, as a result, there is a sense of solidarity among the women to pull each other up and work together in the fight against polio.
From the senior member of the polio programme to the district-level polio officer (who chooses to remain anonymous for her own security), and for so many women in between, being part of the polio programme is not just a job, but a way to work together and support each other.
Dr Rehab Kambo—International Focal Point and Head of the Polio Programme, The World Health Organization, Garowe, Somalia
Dr Rehab Kambo wears two hats at The World Health Organization (WHO): International Focal Point and Head of the Polio Programme in the satellite office at Garowe, Puntland state of Somalia. After joining the polio programme, Dr Rehab set out to understand the context she was working in and one of the things she learned was about the strength of Somali women.
“It is easy not to notice that Somali women are stronger than men in their society, until you spend time with them,” she said.
For Dr Rehab, this realization was driven home on an early assignment. She and a colleague were conducting a surveillance review in a region known as Mudug. Dr Rehab had traveled to Galkacyo by road for eight hours during an active clan conflict, which was no easy feat. Movement was challenging, and the women had to travel with armed escorts. But they were determined, Dr Rehab explains, and they were on a mission.
The two visited transit points at the airport and health facilities to meet with Village Polio Volunteers, who serve the polio eradication initiative at the district level. Upon completing the mission, she and her colleague were elated. Dr Rehab looks back on this as one of the most satisfying – albeit stressful – experiences of her life as a polio eradicator.
Since then, Dr Rehab has taken on the challenge of two roles in one of the most operationally demanding regions in the world. For Dr Rehab inspiration comes easily from the women around her.
“In many instances, they are powerful, independent, and are decision-makers in their families,” said Dr Rehab of the Somali women. Even as a relatively privileged, educated woman, Dr Rehab admits there is a lesson in here for her, and for other women like her.
“Women are so strong, honestly. They can adapt to any role for the good of others,” she said.
Mira A—District Polio Officer, Somalia
Life in Somalia has been extraordinarily difficult since war broke out in 1991, and there is no doubt that it has been harder for women than for men. With an average fertility rate of 6.6 per woman, and high death rates in mothers – one out of every 12 women dies due to pregnancy complications – women are in need of timely and quality health services. A lack of education compounds the problem.
“Despite the challenges, women in Somalia have resiliently stood up to the task and engaged in small-scale businesses over the years to earn a living for their families,” said Mira A, a District Polio Officer in Somalia (we are not using her real name for security reasons).
For Mira A and women like her, taking work outside the home is a way to support not just their families, but themselves – and each other.
“Many women have no time to continue their education or look for other jobs, as they are so busy trying to earn money with their existing means,” she said.
When Mira A looks at the women around her, she sees that education is only part of the answer.
“There is a small sector of women who have managed to earn formal education, but even they do not earn money in most cases. They stay at home and look after their homes and children. Even they need to be empowered, even if it is just to help other women.”
Polio eradication efforts are as much rooted in the social realities as they are in the technological tools. The success of the Global Polio Eradication Initiative comes down to one simple action: the knock on the door, when the child’s caregiver greets the health worker.
Why do caregivers let vaccinators enter their homes? The caregiver’s decision to vaccinate is influenced by many moving parts: social, cultural, economic, and religious. Women health workers and leaders are able to transcend many of these boundaries as they are not only health workers; they are members of that community – someone’s neighbour, friend, aunt, cousin or grandmother.
Polio-endemic, at-risk, and outbreak countries regularly engage women as health officials in immunization activities, constituting about 68% of the frontline workforce. In Nigeria, 99% of frontline workers are women, followed by 56% in Pakistan and 34% in Afghanistan. But their strength in numbers is not the only reason why women are crucial to polio eradication efforts, they are, in fact, behavioural change agents.
Here’s a look at some of the resilient and inspiring women working to eradicate polio in their communities – in their own words:
“Face-to-face interaction is of great significance in polio eradication. I have to walk for miles to sometimes reach only one child during the immunization campaigns. But, hope is essential in eradication efforts as the promise of a better future softens the present-day difficulties.”
Bibi Ayesha — Field Communication Worker, Kandahar, Afghanistan
“As a woman I can easily go to people’s houses and speak to mothers directly about their concerns. I help them with their babies and bring them out to the vaccinators or sometimes vaccinate from the comfort of their homes.”
“It’s important for people to know that there is no alternative to polio vaccination.”
“Assessment skills help me ascertain behaviours of the individuals and communities. Good communication skills help me in solving day-to-day problems…I request them (people) to support female polio teams and get their children vaccinated.”
Julia Kimutai—Sub County Community Strategy Coordinator, Nairobi, Kenya
“There are a lot of myths and misconceptions about the vaccine. To convince some mothers was not easy... but as a woman I think it is simple. Everyone wants to listen to a woman. I have three children—I think being a mother also changes how I can do my job. It gives me skills that you would never get through any training.”
Shamim—Community Health Worker, Balochistan, Pakistan
“In my community, mothers usually ask questions about the polio programme, especially the polio vaccine. To create awareness, I am using a combination of communication and facilitation skills. When community starts group discussion, I make sure that every person, especially mothers, feel included.”
“I think people need to know that working as a frontline worker is not an easy task for women. We also have dreams to support our community…we are also playing an important role in polio eradication.”
Since polio was confirmed in Somalia in late 2017, health authorities have led a complex response to twin outbreaks of circulating vaccine-derived poliovirus type 2 and type 3 (cVDPV2 and cVDPV3), paying special attention to high-risk populations: nomads, internally displaced people (IDPs), and people living in peri-urban slums and rural areas.
So far, five of Somalia’s 12 infected children are from nomadic communities, and another four are from internally displaced families living in urban areas. To boost immunization among eligible children in these populations, vaccination activities have placed a special focus on reaching these communities.
Somalia has a rich culture of people leading pastoral lifestyles, raising livestock and moving with them as the seasons and the weather change. Nomadism has a long history in Somalia and nomads have a special place in Somali society: almost a third of Somalia’s people are nomads. However, they do not observe formal international borders – just like the poliovirus. For health workers, this context poses a significant challenge: How can you be sure you have vaccinated every last child when so many children are on the move?
For health workers, this means searching for polio symptoms in more than 900 health facilities across the country, as well as nutritional centres, camps for IDPs, and key sites along Somalia’s borders. At transit points, along borders and at water collection points, polio teams work to vaccinate children moving in and out of areas experiencing conflict or with limited access to health services. In high-risk areas, the Somali Government, WHO and UNICEF hire local vaccinators – people known and trusted by their communities – and when additional security is necessary, polio partners provide it.
Gaining high-level political goodwill
Even in an emergency, cross-border collaboration is not always easy to come by. In the Horn of Africa outbreak, regional collaboration moved into high gear in September, when health ministers from across the region and representatives from the Intergovernmental Authority on Development (IGAD) countries came together in the Kenyan town of Garissa to reiterate their commitment to ending polio.
One of the event’s key messages was around the risks posed by the easy and frequent mobility of communities across borders. Kenya’s national polio immunization ambassador, former UN Person of the Year and polio survivor, Harold Kipchumba, spoke directly to the pastoral communities in the region.
Kipchumba highlighted their focus on vaccinating animals, and urged parents in these communities to use the same vigour to vaccinate their children against polio, so they are able to serve as future herders for their families.
A regional response to support high-risk populations
The Technical Advisory Group, an independent body of experts that monitors outbreaks and offers guidance, recommended that countries in the region strengthen their coordination. In response, the Horn of Africa Coordination Unit coordinates joint responses among HoA countries – work that includes monitoring current outbreaks, and collaboratively planning, mapping, conducting immunization campaigns and communicating with various audiences. This ensures that countries work together in partnership rather than in silos, viewing the outbreak as one epidemiological block.
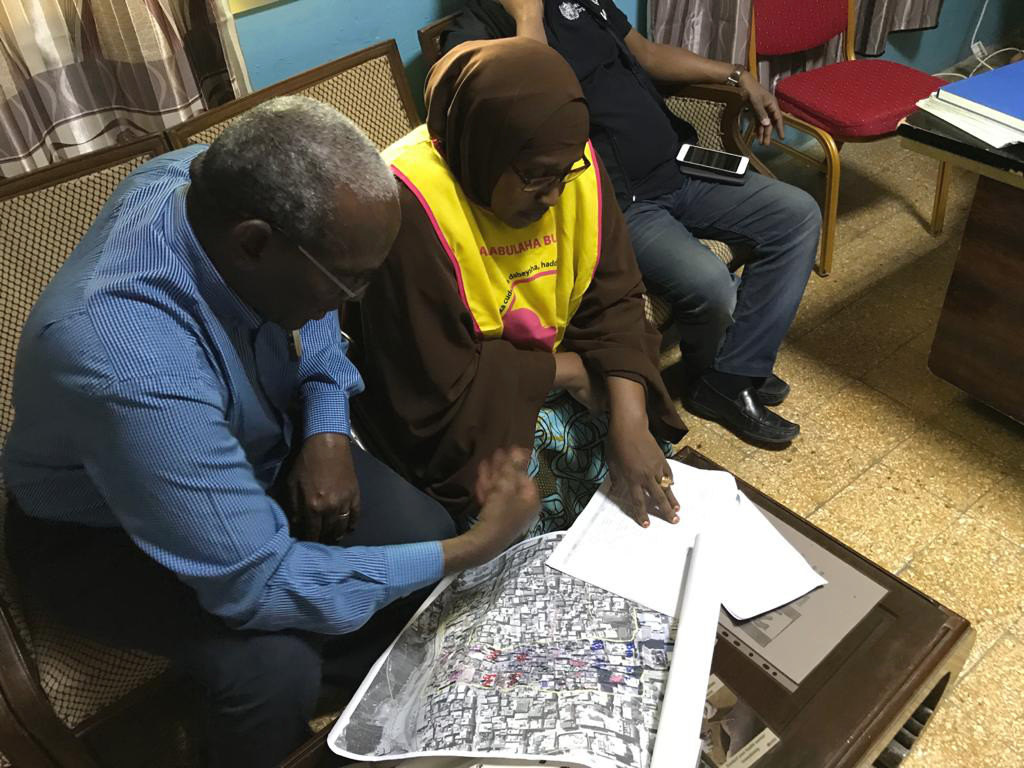
At regional and district levels, teams have spent the last few months building records of every settlement in their area, by lifestyle (nomad, IDP, peri-urban slums, rural). The highest priority: locating special populations – internally displaced persons, refugees, nomadic families, people living in informal settlements in urban areas and communities living in access-compromised areas – in order to reach them with vital polio vaccine.
A vital step in reaching more children, particularly those on the move, has been to move away from paper records and use electronic tools to collect data on children reached and missed during campaigns. This gives data specialists and decision-makers timely, accurate information, allowing them to analyze data in real time and flag areas with where high numbers of children are missed, so teams can revisit these households the following day.
Getting vaccines to the doorstep is not the only challenge for polio eradication teams in Somalia. Parents and caregivers also need information to ensure their children are vaccinated – something Kipchumba spoke to. On rare occasions, vaccinators meet families unconvinced of the need for vaccinations, particularly when the family has a newborn child or a sick child. In the lead up to every campaign, teams of social mobilizers, sometimes joined by influential Islamic leaders or scholars, visit communities to alert them of dates of polio immunization campaigns and the benefits of vaccination. Here, too, special attention is paid to nomadic communities, as polio teams liaise with elders from these communities in order to learn more about these communities and their needs, and to inform community members in appropriate ways about immunization dates and benefits of vaccination.
Left: Shire gives child two drops of the oral polio vaccine to protect them against lifelong paralysis Right: Shire works with vaccination teams to prepare cold boxes to carry polio vaccines
I have spent nearly my whole career working on eradication programmes – first smallpox, then polio. Eradication has been a rewarding career for me because I am so curious to know what is happening in the world. Every time I see a disease that we have worked so long to stop returning, I become so unhappy and know I need to work to stop it.
I worked for the smallpox eradication programme back in the 1970s. I was an epidemiologist – this means that my job was to track the disease and plan how we could stop it.
We used to hold vaccination campaigns at night because then we knew everyone would be at home, and we wouldn’t risk missing a single person. As our cars pulled up out of the dark, people would peer out of their houses to see what was happening. Somalis are very curious! As we brought them the vaccine, occasionally someone would make trouble, but mostly people were pleased to see us.
Somalia was the last country where smallpox was found in the whole world. When I knew we had really ended it in 1977, I was so happy. My name was printed there on the certification document – it was something to be proud of. We had freed the world from smallpox!
I remember one of my friends calling me in 1997 to tell me we were going to eradicate another disease, and that we had to look out for something called ‘AFP’. I thought to myself, what is this ‘AFP’? I hadn’t heard of it. They explained to me that it means acute flaccid paralysis – and that it was the symptom of a disease called polio.
Then one day in 1999, I received a call asking if I would come and work for the second eradication programme in my single lifetime. They said, “If you are ready, we will make you a coordinator. We don’t know if there is polio in Somalia or not, but we want you to come and see.” I jumped at the chance.
We started to search, looking for AFP cases, to collect stool samples and then to send them to the laboratory for testing. And soon, we had confirmation that polio was in Somalia. As soon as we found cases, lots of people came from inside and outside Somalia to help.
By 2002, we found the last case of indigenous polio, and thought the game was won. I even joked to my friends saying, what will we do now that polio is eradicated? They said to me, no – we still have polio in Nigeria, Egypt, Pakistan, many other countries – another case will come. We have to be prepared to stop it if it comes.
And true enough, we had an outbreak in 2005, and again in 2013. Each time we stopped it. Last year, we found circulating vaccine-derived poliovirus type 2. Vaccine-derived polio causes paralysis just like wild polio, and we must eradicate it too.
We started to organize ourselves and held two vaccination campaigns. But then we found another virus – circulating vaccine-derived poliovirus type 3. So now, we are responding to two outbreaks that need different vaccines at the same time. If we miss cases and miss getting vaccines to all children, we can’t stop polio. It is hard, but we will end these outbreaks just as we ended wild polio before.
Eradicating polio has been very difficult – more difficult than it was to end smallpox. I suffered – me and my wife were even kidnapped once. But I am always motivated to keep going. My motivation was never my salary – to stay alive, I need to work. I must know what is going on in my country, if my people are safe. From morning until night, my job is to make sure activities can go on peacefully. My family are my true reason for committing my life to eradication. I have seven children, and 30 grandchildren; I never once missed getting any of them vaccinated. Never.
I am sure that we will finish this job. When we eradicate polio, I will be so happy – I will have been involved in the certification of the second human disease ever to be eradicated. I feel so lucky to have spent my life working for these two eradication programmes; I am proud to tell stories to my grandchildren of my life’s work.
Eradicating polio won’t take a miracle. It is a job. It needs a lot of hard work to end an outbreak. There is no other way – the only way is to work hard, to find cases, and to respond. We hope that in the coming months we will make it. I do believe we will make it. Inshallah.
“Ali was a humble, simple person. He had talent – real talent – in communicating the importance of vaccines to people in his community and around Somalia. He was seen by many as a hero.”
This is how Mahamud Shire, a long-time collaborator of the World Health Organization in Somalia, remembers the late Ali Maow Maalin.
Ali was the last person in the world to be infected with naturally occurring smallpox. After contracting the virus, he decided to devote his life to improving health through vaccination. He did so until his sudden passing in his home district of Merka on 22 July 2013. At the time, he was still serving with WHO as a district polio officer as part of the global polio eradication programme. He was 59 years old.
2018 marks five years since Ali’s passing. This article is being published to commemorate his life and achievements.
Smallpox
Ali Maow Maalin was born in 1954 and worked as a hospital cook. Aged 23, he contracted the smallpox virus.
Although he had previously worked as a vaccinator in the smallpox eradication programme, he himself had not been vaccinated. Fearing the needle, he had avoided the shot by holding his arm when vaccinators came to visit, pretending he had already been inoculated.
“I was scared of being vaccinated then. It looked like the shot hurt,” Ali would later recall when asked why he wasn’t immune on the day the smallpox virus caught up with him.
A man carrying two smallpox-infected children from a nomad encampment had been driving all day, looking for the local isolation camp. Taking wrong turn after another, he finally decided to stop and ask for directions. He did so at the hospital where Ali worked.
“Ali didn’t think about it twice – he jumped in the van and immediately offered to accompany the driver,”
Mahamud tells us. The driver then asked Ali if he had been vaccinated, but Ali simply said: “Don’t worry about that. Let’s go.”
It only took 15 minutes for Ali to contract the virus. Luckily, the form he caught was the less virulent one – variola minor – although still potentially lethal.
Nine days later, Ali started feeling sick.
Making history
Ali’s infection did not lead to a new outbreak. This was primarily because once the hospital where he worked found out he was sick, he was told to stay home. In the meantime, the hospital stopped accepting patients while everyone inside was being vaccinated and quarantined.
A 2011 WHO publication reports how a special team set out to vaccinate everyone in the 50 houses around Maalin’s home. Over the course of two weeks, a total of 54 777 people were vaccinated.
Effectively isolated, the virus didn’t spread. Smallpox was officially declared eradicated in 1979.
This was the first time in history that a major disease had been completely destroyed by human endeavour.
After sickness – a lifelong commitment to polio eradication
After recovering, Ali decided to commit his life to the eradication of another major disease: polio.
Beginning his new role as a vaccinator, he was determined that his own encounter with smallpox would serve as a powerful reminder of why immunization is so important.
“When I meet parents who refuse to give their children the polio vaccine, I tell them my story,” said Ali in 2006. “I tell them how important these [polio] vaccines are. I tell them not to do something foolish like me.”
When we spoke with Mahamud Shire, Ali’s friend and collaborator, we got the unequivocal impression that everyone who crossed paths with Ali, in one way or another, simply liked him.
“He was this really happy person – happy that he was the last case of smallpox still alive, happy that he now had the chance to do his part for his community,” Mahamud says.
Mahamud, who first met Ali in 1977, says Ali’s methods were very successful.
“The way he communicated the importance of vaccination to people – his entire approach – was very effective,” Mahamud says. “He would tell people, ‘I’m vaccinated, and I’ll never get sick’.”
His work, together with that of his WHO colleagues and peers, helped crush Somalia’s polio outbreak in 2005, protecting children from the paralyzing virus.
When Ali suddenly passed away in July 2013, he was still working with WHO through the Global Polio Eradication Initiative, trying to fulfill his quest.
We have never been so close to the final eradication of polio as we are today. When smallpox was eradicated, there were a total of about 52 000 cases each year of wild polio virus. In 2017, only 22 cases of wild poliovirus were reported worldwide.
Now, as with smallpox, the final steps are the most challenging. To eradicate the virus, we must reach every last child with vaccines. We must maintain political and civil society commitment, continue filling immunization gaps, and strengthen disease surveillance in difficult settings.
Ali’s work in communities across Somalia is a reflection of WHO and partner’s long-standing commitment to increasing access to vaccines – everywhere.
One of Ali’s most famous quotes, the one most often used to capture his energy, enthusiasm and firm commitment, is one that puts smallpox and polio one next to the other.
“Somalia was the last country with smallpox. I wanted to help ensure that we would not be the last place with polio too.”
Somalia, which stopped indigenous wild polio in 2002, is currently at risk of circulating vaccine-derived poliovirus type 2, after three viruses were confirmed in the sewage of Banadir province in January 2018. Although no children have been paralysed, WHO and other partners are supporting the local authorities to conduct investigations and risk assessments and to continue outbreak response and disease surveillance.
Underpinning these determined efforts to ensure that every child is vaccinated are local vaccinators and community leaders – nearly all of whom are women.
Bella Yusuf and Mama Ayesha are different personalities, in different stages of their lives, united by one goal – to keep every child in Somalia free from polio. Bella is 29, a mother of four, and a polio vaccinator for the last nine years, fitting her work around childcare and the usual hustle and bustle of family life. Mama Ayesha, whose real name is Asha Abdi Din, is a District Polio Officer. She is named Mama Ayesha for her maternal instincts, which have helped her to persevere and succeed in her pioneering work to improve maternal and child health, campaign for social and cultural change, and provide care for all.
Protecting all young children
Working as part of the December vaccination campaign, which aimed to protect over 700 000 children under five years of age, Bella explains her motivation to be a vaccinator. Taking a well-deserved break whilst supervisors from the Ministry of Health and the World Health Organization check the records of the children so far vaccinated, she looks around at the families waiting in line for drops of polio vaccine.
“I enjoy serving my people. And as a mother, it is my duty to help all children”, she says.
For Mama Ayesha too, the desire to protect Somalia’s young people is a driving force in her work. A real leader, she began her career helping to vaccinate children against smallpox, the last case of which was found in Somalia. Since then, she has personally taken up the fight against female genital mutilation, working to protect every girl-child.
She joined the polio programme in 1998, working to establish Somalia as wild poliovirus free, and ever since to oversee campaigns, and protect against virus re-introduction. In her words, “My office doesn’t close.”
Working in the midst of conflict
The work that Bella and Mama Ayesha carry out is especially critical because Somalia is at a high risk of polio infection. The country suffers from weak health infrastructure, as well as regular population displacement and conflict.
For Bella, that makes keeping children safe through vaccination even more meaningful.
“Through my job I can impact the well-being of my children,” she says. “For every child I vaccinate, I protect a lot more”.
Mama Ayesha echoes those words when she contemplates the difficulties of working in conflict. For most of her life, the historic district where she works, Hamar Weyne, has been affected by recurrent cycles of violence and shelling. With her grown children living abroad, she could easily move to a more peaceful life. But she chooses to stay.
“This is my home, and this is where I am needed. I am here for my team, and all the children.”
Looking up at a picture of her husband, who died many years ago, Mama Ayesha considers the determination and courage that drives her, Bella, and thousands of their fellow health workers to protect every since one of Somalia’s children. Behind her thick wooden desk, she is no less committed than when she began her career. “If I had to do it again it would be my pleasure.”
Bella has a similar professional attitude, combined with the care and technical skill that make her a talented vaccinator. Returning to her stand below a shady tree, she greets the mothers lined up with their children. As she carefully stains the finger of the first small child purple, showing that they have been vaccinated, she grins.
“I am the mother of all Somali children. I am just doing my job”.
Status: affected by circulating vaccine-derived poliovirus type 2 (cVDPV2)
Polio this week in Somalia
No cVDPV2 case was reported this week. There have been three cases reported this year and eight cases reported in 2023.
No cVDPV2-positive environmental sample was reported this week.
International Health Regulations
Somalia is classified by the International Health Regulations (IHR) as a state infected with cVDPV2, with or without evidence of local transmission. It is therefore subject to Temporary Recommendations issued by the International Health Regulations Emergency Committee on Polio Eradication (issued as of August 2023).
Travel advice
WHO’s International Travel and Health recommends that all travellers to polio-affected areas be fully vaccinated against polio. Residents (and visitors for more than 4 weeks) from infected areas should receive an additional dose of OPV or inactivated polio vaccine (IPV) within 4 weeks to 12 months of travel.
The Organization of Islamic Cooperation has celebrated the efforts of its Member States to eradicate polio and is working to ensure that eradication remains at the top of national health agendas. In a resolution passed at the sixth session of the Islamic Conference of Health Ministers, held in Jeddah in early December, the Organization of Islamic Cooperation recognized the importance of ensuring that all children are consistently reached and vaccinated with the polio vaccine. It also highlighted the critical roles of Government leaders and the Islamic Advisory Group in the effort to put an end to the crippling disease.
The Jeddah Declaration
In the Jeddah Declaration, signed by representatives from all Member States, the Organization of Islamic Cooperation reiterated health as one of the basic rights of every human being and reaffirmed their belief that “… the right to health must be at the core of the global agenda.” They reiterated their support to polio eradication and to the full implementation of the Polio Eradication and Endgame Strategic Plan, and recognised the efforts of their Member States to stop transmission. In particular, members were called upon to support the work of the remaining polio endemic countries – Afghanistan, Nigeria and Pakistan – and for the Islamic Advisory Group to continue their work to support the Global Polio Eradication Initiative. The resolution issued at the end of the conference also called upon Member States and other donor entities to provide the necessary financial support that would allow the Islamic Advisory Group to continue its work.
High level support in action in Somalia
Just days after the commitment of member states was reemphasised, the Minister of Health of Somalia Dr Fawziya Abikar Nor showed her commitment to eradication by attending a polio vaccination campaign, alongside Dr Ghulam Popal, WHO Representative for Somalia. High level government commitment has been one of the most important components of eradication in some of the most challenging countries around the world.
Vaccinators attended celebrations to help mark the three years polio-free in Somalia. The event took place at the General Kahiye Police Academy in Mogadishu on August 13, 2017. UN Photo / Omar Abdisalan
This week marks a milestone occasion for Somalia – three years since the detection of the last case of poliovirus in the country. With significant commitment and hard work, Somalia has effectively raised population immunity to the virus, and improved disease surveillance to help pick up any trace of the disease.
Speaking at a celebratory event in Mogadishu, WHO Regional Director for the Eastern Mediterranean, Dr Mahmoud Fikri, has praised Somalia’s efforts to rid the country of the virus, but emphasised the importance of continued attention and focus to keep the country polio free.
“The absence of cases of polio in Somalia today is testament to the leadership, commitment and hard work of the Government and people of Somalia, and the effective support and collaboration of many partners,” Fikri said. “We need to remember however, that Somalia is at risk of reinfection and we must stay vigilant,” he said.
Gaps in vaccination and disease surveillance create an environment where polio can hide and thrive, particularly in countries where health systems are under strain. While the virus exists anywhere, children everywhere are at risk. Countries must remain committed to improving vaccination and disease surveillance activities to achieve eradication and keep the world polio free.
The polio eradication programme is using technology in innovative ways to map the activities of polio workers on the ground, and ensure that expertise and support is getting to the areas where it is most needed.
More than 300 international consultants are deployed by the partners of the GPEI in some of the countries most vulnerable to polio. By strengthening surveillance, tracking the virus, identifying immunity gaps and supporting vaccination campaigns to fill them, these consultants provide an important boost to capacity in polio-affected or vulnerable countries. By using new technologies, the programme is mapping the activities of all consultants to capture the range of locations they travel to and the activities they carry out. These innovations ensure that countries receive the best support from these consultants, and that they are working where the need is greatest.
Survey 123
The introduction of this new technology means that each week, no matter where they are in the world, international consultants report on their activities using a smartphone application called Survey123. The report only takes a minute to complete, works offline and captures their location at the time of reporting. By answering questions on what activities and diseases they have been working on that week, this tool enables the GPEI to capture data in real-time and ensure international consultants are being efficiently deployed in high risk polio areas and being used to their greatest advantage.
In the below snapshot from the first week of October, reports from the consultants can be seen in Guinea, the Lake Chad region, Madagascar, Somalia, Afghanistan and Pakistan – the areas that are most vulnerable to the virus.
From the 3 – 9 October, 242 out of 300 users completed an activity report using Survey 123, giving the programme essential information about their location and activities. Over 5000 reports were captured between February and September.
Getting people where they are most needed
Survey123 is also enabling the GPEI to identify changes in deployment over time. The recent notification of wild poliovirus in the Lake Chad region demonstrated the use of this clarity, by showing the movement of consultants into and around the Lake Chad region, despite insecurity and inaccessibility.
In depth analysis such as this provides greater clarity on what additional human resources are needed to respond to outbreaks or newly recognised risk areas, and indicates how rapidly GPEI resources can be used to fill important needs.
Following cases of polio being found in Nigeria in July 2016, Survey 123 was able to show the movement of international consultants into the affected areas to strengthen the response effort.
The broader benefits of polio eradication
Due to the scale of polio eradication activities even in the most remote and vulnerable areas to reach every last child, international consultants are sometimes present where other health infrastructure is weak. The capacity of the polio programme in these vulnerable areas is sometimes used to support other health initiatives, including improving routine immunisation, measles activities, communication for development and emergency response.
Analysing the collected reports from Survey 123 is giving us greater insight into the extent to which consultants are supporting other health programmes. The support provided to other health programmes shown in the map below highlights the continued benefits of the polio eradication infrastructure to other public health initiatives, giving the donors to the GPEI more bang for their buck when investing in polio eradication. The information gathered from this new technology is helping to inform transition planning efforts, providing information needed to country governments and GPEI partners as they look ahead to what should happen to the polio eradication infrastructure once the goal of a polio-free world has been achieved.
International consultants working on polio are also helping to support other health programmes. This map shows the amount of time in the different WHO Regions being spent on both polio and non-polio activities.
The Global Polio Eradication Initiative (GPEI) is highlighting the innovations that are helping to bring us closer to a polio-free world. Find out about other new approaches driving the polio eradication efforts by reading more in the Innovation Series.
The Puntland Health Ministry/UN agency convoy on the road to Jeriban District to investigate the polio outbreak. @UNICEF Somalia/2014
24 July 2014 – PUNTLAND, Somalia: UN agencies in Somalia combined forces once again to help a joint UNICEF and WHO team visit a remote district of Puntland in north east Somalia where four people have contracted polio this year.
The victims – a young father who died and three children who were paralysed – all came from Jariban district, a long drive on a dusty track from the nearest main town Galkayo in an area known for pirates and armed gangs. As these were the only four polio cases in Somalia so far this year, it was essential to visit the area to discover how the virus got there and how to stop it spreading further. However the terrain, distance, logistics and above all security concerns made it an extremely challenging proposition.
After coordination and cooperation involving at least four UN agencies, the convoy set off on at dawn on 22 July and drove seven hours from Galkayo to Jariban town, where the team met a group of elders to discuss the outbreak and raise awareness. The town has only one Mother and Child Health clinic run by the Red Crescent Society but no hospital or other facilities. The following day they drove another three hours to Towfiq village where they visited the family of the 29 year old man who had died after contracting polio.
‘This was a very sad visit – the man’s wife said she and their five children had been vaccinated but he had not. He was the only breadwinner in the family,’ said Dr. Abraham Mulugeta, WHO Somalia’s Polio Team Leader.
The three children who were paralysed by polio this year live in villages close to Towfiq that are only accessible on foot, so the team could not visit them. However experts had already met one of the children, two year old Asha, who had earlier been brought by her mother who was desperate for help to Galkayo.
While in Towfiq, the team watched the door to door vaccination campaign for children – the third round of vaccinations since the outbreak was discovered in the area in May this year. There will be another campaign in August in the whole of Mudug region and surrounding areas, for adults as well. There is no health facility in Towfiq so these campaigns are crucial to stop the virus spreading.
Vaccinators have been selected from the local community, and clan leaders and elders are being informed about the need for vaccination. More volunteers have been recruited to search actively for any cases of paralysis so that any polio can be swiftly found and the community adequately protected.