It is with deep sadness that we announce the sudden and tragic passing of Dr Chukwuemeka Agbo, Polio Technical Officer, on Sunday, 9 June 2024, in Amman, Jordan.
Known by colleagues and friends as Emeka, 45, was a valued member of the WHO workforce for the last ten years, supporting immunization, polio eradication, and Ebola outbreak response in the African and Eastern Mediterranean regions.
Emeka had recently joined the Polio Eradication team in Amman and in a short time made important contributions as the Regional Incident Support Manager for response to polio outbreaks in Sudan and Djibouti.
Prior to joining the Polio Eradication Programme in Amman, Emeka served as the GPEI Coordinator for Kenya where he managed the response to cholera and polio outbreaks. From February 2022 to December 2023, he served as the GPEI Coordinator in Malawi where he led the outbreak responses to the importation of wild poliovirus type 1, measles and cholera. Over a period of 10 years serving WHO and the Gates Foundation, Emeka successfully led large scale responses to disease outbreaks in the Horn of Africa.
Prior to joining WHO, Emeka worked in the private sector and with a non-profit organization as a medical officer in the Netherlands and Nigeria.
Colleagues across the Organization who have worked with him describe him as humble, energetic, considerate, kind and passionate about his work and a star performer. Emeka saw the work he did as a service. He lived and breathed WHO’s values, serving communities facing complex health and humanitarian crises with compassion. During his short time in Amman, he made deep connections with his colleagues who will miss him dearly.
Emeka is survived by his wife and three children who he loved dearly.
We are in touch with his family and are extending the deepest condolences from the entire WHO family.
Dr Tedros Adhanom Ghebreyesus, WHO Director-General and Dr Hanan Balkhy, WHO Regional Director for the Eastern Mediterranean
A key priority in 2023 is to end both wild- and variant polio transmission around the world is focusing on the most consequential geographies where children are at the highest risk of encountering and spreading the virus, and which collectively accounted for 90% of all new polio cases worldwide in 2022. Northern Nigeria is one of these seven subnational areas that now hold the key to a polio-free world.
In Nigeria increased vaccination and surveillance efforts have yielded positive results in 2022: No isolates from the country’s main historical transmission chain, the Jigawa lineage, which was responsible for most cases and international spread to many neighbouring countries in West Africa, have been detected since February 2022. There was a decline from 1028 cases as on 31st December 2021 to 168 cases as on the 31st December 2022. As a result, the virus is currently confined primarily to two states in the northwest zone of the country, namely Sokoto and Zamfara. This presents a distinctive opportunity for Nigeria to interrupt transmission by December 2023, according to the Expert Review Committee for Polio Eradication and Routine Immunization (ERC), the independent technical group advising the country on its eradication efforts.
In February 2023, the ERC convened its 39th meeting in Nigeria to make recommendations aimed at interrupting transmission of variant type 2 polio and maintaining its indigenous wild poliovirus-free certification status along with the entire African Region. Led by the Ministry of Health’s National Primary Healthcare Development Agency and supported by GPEI partners, Nigerian civil society and Rotarians across the country, efforts are intensifying to fully implement the National Polio Emergency Action Plan (NPEAP).
The country has developed a comprehensive National Polio Emergency Action Plan (NPEAP) to address the risks of all poliovirus types in order to ensure Nigeria and the entire Region’s certification status is maintained, within the context of the political transitioning process, the impact of COVID-19 on the national health systems and economy as well as the increasing concerns of insecurity affecting surveillance and vaccination reach. All recommendations made by the ERC are aimed at aligning the NPEAP with the 2022-2026 Global Polio Eradication Initiative (GPEI) Polio Eradication Strategy.
The ERC noted that the proposed activities for 2023 are contingent on three critical enablers, namely the global stockpile of novel oral polio vaccines (nOPV2) and bivalent oral polio vaccines (bOPV), constraints in financial resources, and a smooth political transition to drive political commitments at sub-national levels. Given the impact of variant type 2 poliovirus over the last few years, there should be limited room for complacency to reach the finish line for the interruption of these strains. The ERC, therefore, called on all partners to support the implementation of the NPEAP for 2023.
The conference also highlighted some of the achievements made in the fight against polio in Nigeria. The conference also highlighted some of the achievements made in the fight against polio in Nigeria. In 2022, there was an 84% decline in variant type 2 poliovirus cases, reduced from 415 cases in 2021 to 48 in 2022. The quality of Supplemental Immunization Activities (SIAs) improved, especially in the last quarter of 2022, and there were narrowed surveillance gaps at sub-national levels. Routine immunization (RI) coverage also improved from 33% in 2016 to 57% in 2022, and COVID-19 vaccination was also optimized to improve demand generation and delivery of other essential immunization vaccines.
The ERC made recommendations in nine thematic areas to fully implement the National Polio Emergency Action Plan, including by continuing to strengthen surveillance, mitigate risks due to inaccessibility and insecurity, build a more resilient routine immunization programme, assure solid vaccine management and advocate for a polio-free Nigeria.
In conclusion, 2023 is a critical year for polio eradication efforts in northern Nigeria and the other most consequential geographies for poliovirus transmission. The global community must continue to support these efforts to ensure that no child is left behind, and we can finally achieve a polio-free world.
April 2022 – Convening this month in Geneva, Switzerland, the Strategic Advisory Group of Experts on immunization (SAGE), the global advisory body to the World Health Organization (WHO) on all things immunization, urged concerted action to finish wild polioviruses once and for all.
The group, reviewing the global wild poliovirus epidemiology, highlighted the unique opportunity, given current record low levels of this strain. At the same time, it noted the continuing risks, highlighted in particular by detection of wild poliovirus in Malawi in February, linked to wild poliovirus originating in Pakistan.
On circulating vaccine-derived poliovirus (cVDPV) outbreaks, SAGE expressed concern at continuing transmission, in particular in Nigeria which now accounts for close to 90% of all global cVDPV type 2 cases, as well as the situation in Ukraine, and its disruption to health services, urging for strengthening of immunization and surveillance across Europe. It also noted the recent detection of cVDPV type 3 in Israel in children, and in environmental samples in occupied Palestinian territories, and urged high-quality vaccination activities and strengthened surveillance.
Preparing for the post-certification era, the group underscored the importance of global cessation of all live, attenuated oral polio vaccine (OPV) use from routine immunization, planned one year after global certification of wild poliovirus eradication. To ensure appropriate planning, coordination and implementation, the group endorsed the establishment of an ‘OPV Cessation Team’, to consist of wider-than-GPEI stakeholder participation and ensure leadership on all aspects of OPV cessation.
SAGE will continue to review available evidence and best practices on a broad range of GPEI-related programmatic interventions, including as relevant the increasing role of inactivated polio vaccine (IPV), including in outbreak response and effects of novel oral polio vaccine type 2 (nOPV2), as part of global efforts to secure a lasting world free of all forms of poliovirus.
Dr. Folake Olayinka has spent over 20 years working in public health, including at the frontline of efforts to eradicate polio and strengthen immunization.
“At local levels, where the rubber meets the road, we need to make things work. Frontline health workers should be supported with tools that meet their needs, and training that truly values their insights, local innovations and problem solving,” said Dr. Olayinka.
Today, as a global health leader and former John Snow, Inc. (JSI) Project Director for the USAID-funded MOMENTUM Routine Immunization Transformation and Equity Project, she continues to exchange lessons and innovative strategies from the frontlines with other parts of the world impacted by polio and low immunization coverage.
On August 25, 2020, Nigeria, previously the last stronghold of endemic wild polio in Africa, was officially declared free of wild poliovirus. One of the factors contributing to this success was the ability to provide high-quality capacity building and support to improve health workers’ competencies at all levels of the health system.
“The health workers on the frontlines – particularly the community-based workers, many of whom are women – are the backbone of all of these efforts. They operate under incredible circumstances to ensure that their communities have access to life-saving health services,” said Dr. Olayinka.
Dr. Olayinka began working on polio in 2002 in Nigeria. She worked closely with colleagues at the Nigerian Ministry of Health, the World Health Organization, the EU and UNICEF to ramp up health worker training in support of the Nigerian government’s National Program on Immunization.
Her team’s dedication was remarkable. “We were willing to go everywhere to reach the last child. Once I walked four hours to support an immunization team,” she recalls.
Shaking things up
Dr. Olayinka emphasized training quality and the use of feedback to continuously improve the training experience for health workers. She led the development of numerous training guides and materials for polio eradication and developed the country’s first Basic Guide for Routine Immunization Service Providers. She also worked closely with WHO and EU colleagues to develop the first measles campaign field training materials in Nigeria.
Knowing that training of health workers must be continuous, she introduced mentoring as an important post-training approach in Nigeria’s immunization program.
“We needed to move people towards a more interactive approach,” said Dr. Olayinka. “These approaches transfer knowledge while maintaining dignity and recognize that people in the global South have something valuable to contribute.”
Recalling her experience training different types of health workers and trying to promote adult learning methods, she said, “I once walked into a room of senior health commissioners from all over the country. The room was filled with the usual PowerPoints, and people were not engaged – even sleeping.”
“When I went to the front of the room for my session, I introduced myself using my first name and explained the more interactive approach that I was proposing for the training. At first people were silent, but as the training went on, they really came alive. They were engaged and now identifying the real issues and generating the types of ideas that could truly change policy and improve services – you could see their passion coming through. I felt the ship took a turn.”
Dr. Olayinka also tackled training needs at the community-level and strongly promoted the use of local languages in the training of frontline health workers, particularly social mobilizers for polio eradication.
“At local level in northern Nigeria, most people spoke Hausa; however, training materials were largely in English at the time, and many of the women who were able to enter the homes to provide polio vaccinations did not understand English.”
“The polio programme was at a crisis point and was also facing a lot of refusals. As people in the region were not receiving other basic health services, they began not to trust polio vaccination efforts as it was one of the only services they were receiving.”
A pivot was needed, with a closer examination of what was working – and what was not – for all aspects of the eradication effort.
“These women were looking for the basics: how do I answer questions from caregivers, how do I provide polio drops, how do I enter my data?” remembers Dr. Olayinka “With this insight, I developed a flip chart using pictures – I even included a photo of my own son receiving the oral polio drops. We also used the local languages, role play, peer to peer methods, and songs as part of the training methodology.”
In the area of routine immunization, Dr. Olayinka worked with her team and other partners to introduce a stronger supervision system. The system included a checklist with clear standards for supervision of routine immunization, as well as a checklist on training quality as part of the pre-campaign preparedness. This helped National Primary Health Care Development Agency staff to provide ongoing support and mentorship for health workers. Many of these approaches and materials are still being used today and are updated periodically.
At the heart of the response, you will find a woman
Dr. Olayinka worked in a particularly challenging environment in northern Nigeria. “There are gender dimensions tightly linked with socio-cultural and deep-seeded religious beliefs in the northern state”, she recalled.
Oftentimes mothers had to seek permission from their husbands before they could allow the children to be vaccinated or access health services. “Even when they understood the value, women did not have decision-making power.”
The polio programme was able to reach women in new ways. Men originally started out as polio workers, but it quickly became apparent they were missing children under five because they were not allowed into homes due to cultural norms. The solution: hire women to go door-to-door and reach populations being missed.
“The polio programme brought women out into the workforce in an unprecedented way, says Dr. Olayinka. “Women were powerful mobilizers, particularly older, respected women and could enter any home. The polio programme was one of the first programmes bringing the women out, training them how to speak to other women and community members, which gave them a standing in the community. They also received some stipends which empowered them a bit financially.”
Many of these women later transitioned to supporting broader immunization and other health efforts in their communities, leading to higher child survival rates and less disease in communities.
“This is part of my passion when I talk about integration – these women in the communities, after getting a start from the polio programme, can be trained to talk about routine immunization, use of long-lasting insecticidal nets to prevent malaria, breastfeeding, WASH etc.”
“As a result of the polio programme they have social capital that can be expanded to improve health outcomes in their communities.”
To women leaders of the future
Dr. Olayinka remains committed to elevating the contributions of frontline health workers operating in challenging situations across the world.
When asked what advice she would give to women beginning their careers in public health, Dr. Olayinka said, “Be persistent and do not give up on your dreams. Even where you face discrimination because you are a woman, be focused and persist. Ensure that you are constantly building your capacity and equip yourself.”
“Women at all levels can make a difference, so take the leap—there are no limits to what you can achieve.”
In 2003, Melissa Corkum received a call that would change her life. The World Health Organization wanted to interview her for a position in their polio eradication team. Like most people who are hearing about polio eradication for the first time, the story compelled her, and she packed her bags to embark on a new adventure. Seventeen years later, she remains a dedicated champion of polio eradication.
A self-proclaimed ‘virus chaser’, Melissa has worked in all three polio endemic countries – Afghanistan, Pakistan and Nigeria. She found inspiration in her first field job in Nigeria, where she realized the scale of the polio eradication programme and that she was a part of something tremendous in public health history.
“I was amazed and inspired when I first saw the efforts of the front-line workers delivering vaccines to the doorstep. It may seem simple to deliver a couple drops into a child’s mouth, but when you see it in motion for the first time, it is truly remarkable,” Melissa said.
To this day, Melissa remains in awe of the work required to make ‘reaching every child’ possible. From mobilizing financial resources, to getting vaccines where they need to be while keeping them cool. From the microplanning to ensure all children and their houses are on a map, to the mobilization of champions in support of polio and immunization. Along the way, the stewards of these processes play an essential role to deliver the polio vaccine.
Melissa has worn many hats during her time in polio eradication, but her current role may be the most challenging yet. As the Polio Outbreak Response Senior Manager with UNICEF, she must answer the formidable challenge of containing outbreaks, using her expertise to inform global policy, strategy and operations.
To do this Melissa spent 80% of her time in the field prior to the outbreak of COVID-19, working with partners of the Global Polio Eradication Initiative (GPEI), Ministries of Health and local health workers.
Her work is a mix of challenge and excitement – the challenges of containing outbreaks, including those affected by the COVID-19 emergency – and excitement in developing new tools and methods to overcome the evolving challenges that present barriers to eradicating polio.
“There is never a dull day no matter what hat you may be wearing within this programme. If we are going to put an end to polio for good, we are going to have to fight the fight on a number of fronts – endemics and now the emerging issue of outbreaks in a post-COVID world,” said Melissa.
“The key is a willingness to do whatever it takes to get the job done.”
At times, Melissa felt the weight of the enormous challenges to eradicate polio, especially during her time in Afghanistan, where protracted conflict has complicated efforts to deliver basic services to the most vulnerable. Melissa often reflects on her time as Polio Team Lead there and the emotional rollercoaster she faced trying to stay ahead of the virus, while watching the tragedy of war unfold in the country.
“But when I felt down, I would pick myself up and get ready to face the next challenge. I found hope and inspiration in the resilience of the Afghan people, especially the women who worked in the polio programme, risking their lives and demonstrating a courage that stood out amidst all the difficulties.”
Melissa sees gender as one of the keys to polio eradication. She firmly believes that the only way to tighten the gaps in the system is by involving and empowering women equally in all roles across the programme, and that the only way to reach every child is to ensure their caregivers are equally informed and engaged in the decision making process.
“Unless we involve more women in the programme in certain corners of the world, we will continue to reach the same children and miss the same children, making polio eradication ever more difficult,” Melissa said.
“Change won’t happen if we don’t change the way we think about involving women. We need to listen to their views and open the doors for more women to join and participate equally from the community level and all the way to the leadership, decision-making level.”
Melissa was born in a small town in Nova Scotia, Canada. Her views on the critical involvement of women and gender equality in the polio programme very much align with her government’s Feminist Aid Policy. The Government of Canada has been a long-time champion of polio eradication and recently generously pledged C$ 190 million to assist the GPEI achieve its objectives of polio eradication.
Greater gender equity is one of the legacies that the polio programme is working to leave behind after eradication. Reflecting on her career, Melissa explains what keeps her working to defeat polio after all these years.
“It is so inspiring to be part of something tangible and something that is completely possible if we commit ourselves to doing everything possible to find every last child”.
The COVID -19 pandemic response requires worldwide solidarity. The Global Polio Eradication Initiative (GPEI) has a public health imperative to ensure that its resources are used to support countries in their preparedness and response. The COVID-19 emergency also means that polio eradication will be affected. We will continue to communicate on impact, plans and guidance as they evolve.
Using the vast infrastructure developed to identify the poliovirus and deliver vaccination campaigns, the polio eradication programme is pitching in to protect the vulnerable from COVID-19, especially in polio-endemic countries. From Pakistan to Nigeria, the programme is drawing on years of experience fighting outbreaks to support governments as they respond to the new virus.
Pakistan
Few health programmes have as much practice tracking virus or reaching out to communities as the Pakistan polio eradication programme. This means the polio team is in a strong position to support the Government of Pakistan in COVID-19 preparedness and response.
Currently, the polio team is providing assistance across the entire country, with a special focus on strengthening surveillance and awareness raising. Working side-by-side with the Government of Pakistan, within three weeks the team has managed to train over 280 surveillance officers in COVID-19 surveillance. It has also supported the development of a new data system that’s fully integrated with existing data management system for polio. All polio surveillance staff are now doubling up and supporting disease surveillance for COVID-19. Through cascade trainings, they have sensitized over 6,260 health professionals on COVID-19, alongside their polio duties, in light of the national emergency. These efforts will continue unabated as the virus continues to spread.
Adding to the capacity of the government and WHO Emergency team, the polio team are also engaged in COVID-19 contact tracing and improving testing in six reference laboratories. They have been trained to support and supplement the current efforts, preparing for a sudden surge in cases and responding to the increase in travelers that need to be traced as a result of the rise in cases. The regional reference laboratory for polio in Islamabad is also providing technical support to COVID-19 testing and has been evolving to cater to the increased demands.
As this is a new disease, polio staff are lending their skills as health risk communicators – providing accurate information and listening to people’s concerns. The government of Pakistan extended a national help line originally used for polio-related calls to now cater to the public’s need for information on COVID-19. The help line was quickly adapted by the polio communication team once the first COVID-19 case was announced. The polio communications team is using strategies routinely used to promote polio vaccines to disseminate information about the COVID-19 virus, including working with Facebook, to ensure accurate information sharing, and airing television adverts. As time goes on, the teams will train more and more people ensuring the provision of positive health practices messages that can curb the transmission of the virus.
Afghanistan
Currently, community volunteers who work for the polio programme to report children with acute flaccid paralysis (AFP) are delivering messages on handwashing to reduce spread of COVID-19, in addition to polio. UNICEF is similarly using its Immunization Communication Network to disseminate information on personal hygiene.
Field staff have taken the initiative of using their routine visits to health facilities, during which they check for children with AFP, to check for and report people who may have COVID-19. Meanwhile, programme staff are building the capacity of health workers to respond to the novel coronavirus.
To coordinate approaches, the WHO Afghanistan polio team has a designated focal point connecting with the wider COVID-19 operation led by the Government of Afghanistan. The polio eradication teams at regional and provincial levels are working closely with the Ministry of Public Health, non-governmental organizations delivering Afghanistan’s Basic Package of Health Services and other partners to enhance Afghanistan’s preparedness.
Nigeria
“In the field, when there is an emergency, WHO’s first call for support to the state governments is the polio personnel,” says Fiona Braka, WHO polio team lead in Nigeria.
In Ogun and Lagos states, where two cases of COVID-19 have been detected, over 50 WHO polio programme medical staff are working flat out to mitigate further spread, using lessons learnt from their years battling the poliovirus. Staff are engaged in integrated disease surveillance, contact tracing, and data collection and analysis. Public health experts working for the Stop Transmission of Polio programme, supported by the US Centers for Disease Control and Prevention, are using their skills to undertake COVID-19 case investigations.
The WHO Field Offices -which are usually used for polio eradication coordination- are doubling up as coordination hubs for WHO teams supporting the COVID-19 response. The programme is also lending phones, vehicles and administrative support to the COVID-19 effort.
In states where no cases of COVID-19 have been reported, polio staff are supporting preparedness activities. At a local level, polio programme infrastructure is being used to strengthen disease surveillance. Polio staff are working closely with government counterparts and facilitating capacity building on COVID-19 response protocols and are working to build awareness of the virus in the community. Specials efforts are being undertaken to train frontline workers as they are at high risk of contagion.
Beyond polio-endemic countries
Trained specialists in the STOP program, part of the Global Polio Eradication Initiative, are actively supporting preparations or response to COVID-19 in 13 countries worldwide. The WHO Regional Office for Africa’s Rapid Response Team, who usually respond to polio outbreaks, are aiding COVID-19 preparedness in countries including Angola, Cameroon and the Central African Republic. Meanwhile, polio staff in other offices are ready to lend support, or are already lending support, to colleagues working to mitigate and respond to the new virus.
In our work to end polio, the programme sees the devastating impact that communicable diseases have. With this in mind, we are fully committed to supporting national health systems by engaging our expertise and assets to help mitigate and contain the COVID-19 pandemic, alongside continuing concerted efforts to eradicate polio.
For the latest information and advice on the COVID-19 disease outbreak visit the WHO website.
In Jere Local Government Area, in Borno State, Nigeria, a team of male surveillance officers have been dispatched to look for the poliovirus.
They make a first stop at the home of Hajiya Liman Bello, a mother of three and a housewife.
“Who are all of you and what do you want?” Hajiya asks.
“We are health workers please. We need to collect stool samples from your children as there has been a case of Acute Flaccid Paralysis (AFP) in this area”, they reply.
Hajiya isn’t comfortable with the idea of a male health worker handling stool sample collection for her children. She requests that surveillance officers return with a female colleague if they wish to go ahead.
Recognising the links between gender and disease surveillance
In line with the Global Polio Eradication Initiative’s gender strategy, Nigeria’s polio programme has been quantifying the gender aspect of its work. While women make up 95% of frontline workers delivering polio vaccines, a 2017 study conducted by the World Health Organization found there were significantly more men than women engaged in polio surveillance activities in Nigeria.
In 2016 there were 29 men employed in Nigeria as state epidemiologists compared with just eight women doing the same job; 23 male state disease surveillance and notification officers (DSNOs) compared with 14 women, and at a Local Government level, 609 male DSNOs versus 218 female.
The results of the study prompted reflection by programme staff. Gender, like other factors such as age, education and socioeconomic status, is an important determinant of health-seeking behaviour and outcomes. In the case of disease surveillance officers, gender diversity amongst personnel helps the programme build trust and acceptance amongst parents.
“I believe gender strongly influences disease surveillance and access to immunization services,” says Dr Kabir Yusuof, a health worker who has worked with the Nigerian Government polio programme for over ten years.
“Nigeria is generally a culturally attuned country. There are some communities where men only feel comfortable with female health workers, especially when it comes to house-to-house outreach and matters of maternal health. For this reason, I believe the role of women in both polio surveillance and response cannot be overlooked.”
Surprisingly, the report showed there were more men than women working as surveillance focal points in health facilities in northern zones of Nigeria, compared to the south. Using gender-disaggregated data helped the programme see where things need to change.
“WHO advocates for breaking…illusions that women cannot ‘fit in’ when it comes to disease surveillance practice,” says Dr Fiona Braka, Team Lead for the Expanded Programme on Immunization at WHO Nigeria.
Polio eradication was the first disease programme at the World Health Organization to develop a dedicated gender strategy. The Nigeria AFP surveillance gender study had never been done before and has helped lay the groundwork for further examination of the programme through a gender lens. The authors of the study found that the number of AFP cases detected in boys and girls was similar, as were polio vaccination rates.
Dr Braka observes, “Integrating or mainstreaming gender into all facets of socio-economic life is key to tackling gender inequalities.”
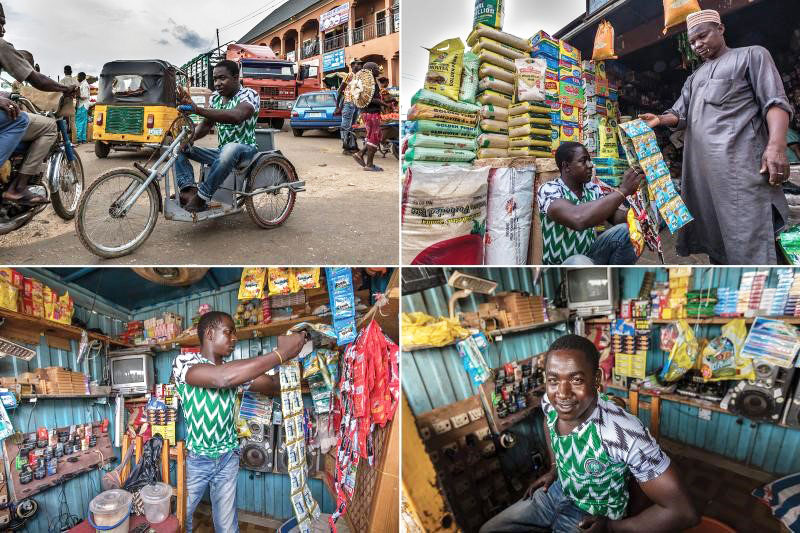
When we talk about PolioPlus, we know we are eradicating polio, but do we realize how many added benefits the programme brings? The ‘plus’ is something else that is provided as a part of the polio eradication campaign. It might be a hand-operated tricycle or access to water. It might be additional medical treatment, bed nets, or soap.
This series looks at the ‘pluses’ that Rotarians worldwide help to provide. Our first article looked at prevention of other diseases, and in part two we investigated how Rotary contributes to clean water provision. In our final article, we consider how Rotarians support those who have contracted polio, and who now live with permanent paralysis.
Creating jobs
Polio paralysis left Isiaku Musa Maaji, who lives in Nigeria, with few ways to make a living. At 24, he learned to build hand-operated tricycles designed to provide mobility for adults and children with physical disabilities, and later started his own business assembling them. His first break came, he says, when his local government placed a trial order. Officials were impressed with his product, and the orders continued.
Rotary’s Nigeria PolioPlus Committee recently ordered 150 tricycles from Maaji to distribute to polio survivors and others with mobility problems. The relationship he has built with local Rotarians has motivated him to take part in door-to-door polio vaccination campaigns.
“It is not easy to be physically challenged,” he says. “I go out to educate other people on the importance of polio vaccine because I don’t want any other person to fall victim to polio.”
Aliyu Issah, another polio survivor, feels lucky; he’s able to support himself running a small convenience store. He knows others with polio paralysis who have attended skills training programmes but lacked the money to start a similar business. In the absence of ready employment, some of them were forced to beg on the street.
He notes however that the polio eradication programme provides a job that is uniquely suited to polio survivors: educating others about the effects of the disease.
“Some of my friends who used to be street beggars now run their own small business with money they earn from working on the door-to-door immunization campaign,” Issah says.
Improving health care
In Maiduguri, Nigeria, Falmata Mustapha rides a hand-operated tricycle donated to her by Rotary’s Nigeria PolioPlus Committee. She is joined by several health workers for a door-to-door immunization campaign, bringing polio drops to areas without basic health care.
UNICEF data show that polio survivors like Mustapha have a remarkable success rate persuading reluctant parents to vaccinate their children — on average, survivors convince seven of every ten parents they talk to. In places where misinformation and rumours have left people hesitant to vaccinate, the survivors’ role in the final phase of the eradication effort is critical.
“Since working with the team, I have seen an increase in immunization compliance in the community,” Mustapha says. “I am well-regarded in the community because of my work, and I am happy about this.”
When we talk about PolioPlus, we know we are eradicating polio, but do we realize how many added benefits the programme brings? The ‘plus’ is something else that is provided as a part of the polio eradication campaign. It might be a hand-operated tricycle or access to water. It might be additional medical treatment, bed nets, or soap.
This series looks at the ‘pluses’ that Rotarians worldwide help to provide. Our first article looked at prevention of other diseases. In part two, we look at another lifechanging intervention: providing clean water for communities.
Providing clean water
Addressing a critical long-term need such as access to clean water helps build relationships and trust with community members. Within camps for displaced people in northern Nigeria, the polio vaccinators who regularly visit communities are sometimes met with frustration. “People say, ‘We don’t have water, and you’re giving us polio drops,’” Tunji Funsho explains. Rotary and its partners have responded by funding 31 solar-powered boreholes to provide clean water in northern Nigeria, and the effort is ongoing.
Supplying clean water to vulnerable communities is a priority of the PolioPlus programme not only in Nigeria, but also in Afghanistan and Pakistan — the only other remaining polio-endemic nations, where transmission of the virus has never been interrupted.
“Giving water is noble work also,” says Aziz Memon, chair of Rotary’s Pakistan PolioPlus Committee.
Access to safe drinking water is also an important aspect of the The Polio Endgame Strategy 2019-2023, which aims to “ensure populations reached for polio campaigns are also able to access much-needed basic services, such as clean water, sanitation, and nutrition.” The poliovirus spreads through human waste, so making sure people aren’t drinking or bathing in contaminated water is critical to eradicating the disease. Bunmi Lagunju, the PolioPlus project coordinator in Nigeria, says that installing the boreholes has helped prevent the spread of cholera and other diseases in the displaced persons camps.
Communities with a reliable source of clean water have a reduced rate of disease and a better quality of life. “When we came [to the camp], there was no borehole. We had to go to the nearby block factory to get water, and this was difficult because the factory only gave us limited amounts of water,” says Jumai Alhassan, as she gives her child a bucket-bath. “We are thankful for people who provided us with the water.”
By looking holistically at the needs of communities, Rotarians are ending polio, and making a significant contribution to overall health.
This story is part of the Broader Benefits of Polio Programme series on our website, which originally appeared in the October 2019 issue of The Rotarian magazine. Read part one.
The polio eradication campaign needs your help to reach every child. Thanks to the Bill & Melinda Gates Foundation, your contribution will be tripled. To donate, visit endpolio.org/donate.
Reposted with permission from Rotary.org When we talk about PolioPlus, we know we are eradicating polio, but do we realize how many added benefits the programme brings? The “plus” is something else that is provided as a part of the polio eradication campaign. It might be a hand-operated tricycle or access to water. It might be additional medical treatment, bed nets, or soap. This series takes a look at the ‘Pluses’, starting with prevention of other diseases. A 2010 study estimates that vitamin A drops given to children at the same time as the polio vaccine had at that time already prevented 1.25 million deaths by decreasing susceptibility to infectious diseases.
We take you to Nigeria, which could soon be declared free of wild poliovirus, to show you some of the many ways the polio eradication campaign is improving lives.
Polio vaccination campaigns are difficult to carry out in northern Nigeria, where insurgency has displaced millions of people, leading to malnutrition and spikes in disease. When security allows, health workers diligently work to bring the polio vaccine and other health services to every child, including going tent to tent in camps for displaced people.
The Global Polio Eradication Initiative (GPEI), of which Rotary is a spearheading partner, funds 91% of all immunization staff in the World Health Organization’s Africa region. These staff members are key figures in the fight against polio — and other diseases: 85% give half their time to immunization, surveillance, and outbreak response for other initiatives. For example, health workers in Borno use the polio surveillance system, which detects new cases of polio and determines where and how they originated, to find people with symptoms of yellow fever. During a 2018 yellow fever outbreak, this was one of many strategies that resulted in the vaccination of 8 million people. And during an outbreak of Ebola in Nigeria in 2014, health workers prevented that disease from spreading beyond 19 reported cases by using methods developed for the polio eradication campaign to find anyone who might have come in contact with an infected person.
Children protected from polio still face other illnesses. In Borno, malaria kills more people than all other diseases combined. To prevent its spread, insecticide-treated bed nets — such as the one Hurera Idris is pictured installing in her home above — are often distributed for free during polio immunization events. In 2017, the World Health Organization organized a campaign to deliver antimalarial medicines to children in Borno using polio eradication staff and infrastructure. It was the first time that antimalarial medicines were delivered on a large scale alongside the polio vaccine, and the effort reached 1.2 million children.
Rotary and its partners also distribute soap and organize health camps to treat other conditions. “The pluses vary from one area to another. Depending on the environment and what is seen as a need, we try to bridge the gap,” says Tunji Funsho, chair of Rotary’s Nigeria PolioPlus Committee. “Part of the reason you get rejections when you immunize children is that we’ve been doing this for so long. In our part of the world, people look at things that are free and persistent with suspicion. When they know something else is coming, reluctant families will bring their children out to have them immunized.”
Rotarians’ contributions to PolioPlus help fund planning by technical experts, large-scale communication efforts to make people aware of the benefits of vaccinations, and support for volunteers who go door to door.
Volunteer community mobilizers are a critical part of vaccination campaigns in Nigeria’s hardest-to-reach communities. The volunteers are selected and trained by UNICEF, one of Rotary’s partners in the GPEI, and then deployed in the community or displaced persons camp where they live. They take advantage of the time they spend connecting with community members about polio to talk about other strategies to improve their families’ health.
Nigerian Rotarians have been at the forefront of raising support for Rotary’s polio efforts. For example, Sir Emeka Offor, a member of the Rotary Club of Abuja Ministers Hill, and his foundation collaborated with Rotary and UNICEF to produce an audiobook called Yes to Health, No to Polio that health workers use.
This story is part of the Broader Benefits of Polio Programme series on our website, which originally appeared in the October 2019 issue of The Rotarian magazine.
The polio eradication campaign needs your help to reach every child. Thanks to the Bill & Melinda Gates Foundation, your contribution will be tripled. To donate, visit endpolio.org/donate.
Since its inception in 1988, the Global Polio Eradication Initiative (GPEI) is driven by a singular purpose: defeat the poliovirus and secure the world from this disease.
While there may be no cure from polio, it is preventable and eradicable. Thanks to global immunizations efforts of national health authorities backed by international partners – WHO, Rotary International, the US Centers for Disease Control and Prevention (CDC), UNICEF, the Bill & Melinda Gates Foundation and Gavi, the Vaccine Alliance — cases of wild poliovirus have dropped from 350 000 in 1988 to 33 cases reported in 2018, and four Regions of the world have been certified free of wild poliovirus.
Another milestone was achieved last week: Nigeria crossing three years without detection of wild poliovirus. With this, the African Region can now possibly start the official process to certify the WHO African Region free of wild poliovirus.
This milestone was a slow and steady win, which would not have been possible without the people who make up the very fabric of Nigerian communities. Trust-building efforts by traditional leaders and the network of women making household visits across the country, made it possible to overcome socio-cultural and operational barriers to vaccination.
Read about the innovative practices for polio eradication in Nigeria.
21 August 2019 marks three years since Nigeria last reported a case of wild poliovirus. This is an important public health milestone for the country and the entire Africa Region, which is now a step now closer to polio-free certification.
At the press conference in Abuja, the Executive Director of the National Primary Health Care Development Agency (NPHCDA), Dr Faisal Shuaib, acknowledged that the three-year mark is an important moment in the fight against polio but also emphasized the need for vigilance ̶ “one which we must delicately manage with cautious euphoria.”
“This achievement would certainly not have been possible without the novel strategies adopted in the consistent fight against polio and other vaccine preventable diseases. We commend the strong domestic and global financing and the commitment of government at all levels,” the Executive Director stated.
Innovation, partnership and resolve have all underpinned advancements made in Nigeria, together with the commitment of tens of thousands of health workers. “Since the last outbreak of wild polio in 2016 in the northeast, Nigeria has strengthened supplementary immunization activities and routine immunization, implemented innovative strategies to vaccinate hard-to-reach children and improved acute flaccid paralysis (AFP) and environmental surveillance. These efforts are all highly commendable,” said WHO’s Officer in Charge for Nigeria, Dr Peter Clement.
However, despite progress, there is still much left to be done. Continued work to reach every last child with the polio vaccine, as well as strengthening surveillance and routine immunization across the region, will be key to keeping wild polio at bay and protecting the gains achieved.
Should there be no more cases in Nigeria or from countries in the Africa Region, and surveillance data submitted by countries meets evaluation criteria, the Africa Regional Certification Committee (ARCC) could certify the Region as wild polio-free as early as mid-2020.
The press briefing was attended by country representatives of all GPEI partners: WHO, UNICEF, CDC, Rotary and the Bill & Melinda Gates Foundation; as well as USAID, Government of Germany, EU and Canada. The Emir of Jiwa, representing the Northern Traditional Leaders Committee was also in attendance.
“Our area is a pretty difficult terrain because we live in the water and it is not easy for the teams coming from outside the community to gain access. So, the (hand-drawn) maps make it possible for us to identify areas we have yet to reach during the immunization exercise”, says Peter Idowu, a veteran community mobilizer and team supervisor in Makoko — a riverine shanty town located on the coast of mainland Lagos city, southwest Nigeria. Native to the village, Peter is the man to go to whenever the polio immunization teams face challenges navigating the waterways or the community.
The sprawling water city Makoko is a slum located across the Third Mainland Bridge on the lagoon. It is a largely low-income community with half the population on water and the other half on land. Informal, makeshift houses with corrugated iron roofs sit precariously atop stilts. Down below, narrow wooden boats act as a form of aquatic taxi ferrying goods and people around the bustling community. Nobody knows the exact population of this slum district of Lagos, but it is estimated to be as high as 100 000. It is mostly a fishing community inhabited by the Egun people.
“My goal is to see that all the kids in our community are immunized and live healthy lives. That is why I engage our teams in sensitizing parents all the time on the importance of routine immunization and the dangers of polio. As a member of the community and with a passion of becoming a health worker myself, I kept on mobilizing our people for easy accessibility, because our language is different from Yoruba and most of the Polio teams can’t speak the language. It is always easy with me being in the Polio team as our people will readily accept the vaccine without rejecting,” says Peter.
Nigeria is the only country in Africa and one of the only three in the world endemic to wild poliovirus, alongside Afghanistan and Pakistan. Nigeria is also affected by circulating vaccine-derived poliovirus type 2 (cVDPV2) outbreaks.
UNICEF works closely together with Global Polio Eradication Initiative (GPEI), key polio partners and the Nigerian government. There is a vast network of over 20 000 community mobilizers focusing on demand creation and improving health-seeking behaviors of caregivers.
“We had not seen vaccination teams in our community for a very long time. Sometimes we go for months without vaccinating our children, if we don’t take our children to the mainland to get them vaccinated”, says Mr. Atebakuro Oton George, a fisherman and father of five, residing in Minibie ward of Nigeria’s Bayelsa State.
A largely riverine state, Bayelsa accounts for over 60% of the delta mangrove of the Niger Delta. Many children here continue to miss their chances at life-saving vaccination, as transport is precarious in the tangle of creeks and rivers that crisscross the state. In 2018 a number of innovative strategies such as, immunization boats at sea and community engagement through the traditional hierarchy and sensitization activities, supported by World Health Organization (WHO) through the Government of Bayelsa were introduced to reach a wider net of children.
“Now on weekly basis, health workers brave the seas and visit our communities to vaccinate our children”, an elated Mr. George continues.
Subsistence farming and fishing are the mainstay of the local population’s economy and diet. Health services are provided by primary health care centers located within the island communities.
“The difficulty of accessing healthcare services is due to suboptimal and expensive coastal and waterway transportation from the distant communities to healthcare centers, hence, innovative strategies are being employed to reach the underserved and vulnerable population with vaccination and other health interventions especially during Supplemental Immunization Activities (SIAs)”, says Dr Edmund Egbe, WHO State Coordinator in Bayelsa.
To reach ‘missed’ children, community engagement activities to increase demand for immunization have been initiated to bolster willingness of caregivers to readily access the interventions even when in the middle of the river or the ocean. The successful implementation of the community engagement framework has resulted in high-level acceptance of immunization services in the State. From April 2018 to April 2019, over 169 836 children received vaccination.
Routine immunization coverage has improved remarkably: the first quarter RI Lot Quality Assurance Survey (LQAS)— a quarterly activity organized by the National Emergency Routine Immunization Coordinator Centre (NERICC) to assess routine immunization performance, reasons for non-immunization as well as efforts to improve uptake and utilization of RI in Nigeria—conducted in April 2019 indicate that the State is second best in the country. Previously, the State was ranked amongst others in the country as poor-performing from the last National Immunization Coverage Survey (NICS) conducted in 2016; this led to the inauguration of an emergency response committee in March 2018.
King Diete-Spiff, the Chairman and the ‘Amanayanbo’ of Town-Brass, in his meeting with the State Traditional Rulers Council said, “Sustaining the innovative strategies of vaccinating vulnerable populations will undoubtedly increase immunity against vaccine preventable diseases and reduce the mortality and morbidity rate in difficult to access communities”. He described the polio infrastructure in Bayelsa, supported by WHO and partners, as the bedrock of driving successful healthcare intervention at the grassroots.
Support for polio eradication and routine immunization to Nigeria through WHO is made possible by funding from the Bill & Melinda Gates Foundation, the Department for International Development (DFID – UK), the European Union, Gavi, the Vaccine Alliance, the Government of Germany through KfW Bank, Global Affairs Canada, the United States Agency for International Development (USAID), Rotary International and the World Bank.
The 72nd World Health Assembly, the governing body of the World Health Organization held by in Geneva, Switzerland is the biggest congregation of public health actors. Taking advantage of the critical mass of global leaders, the Global Polio Eradication Initiative hosted an event for polio eradicators, partners and stakeholders on 21 May 2019.
The event, To Succeed by 2023—Reaching Every Last Child, celebrated the GPEI’s new Polio Endgame Strategy 2019-2023. The five-year plan spells out the tactics and tools to wipe out the poliovirus from its last remaining reservoirs, including innovative strategies to vaccinate hard-to-reach children and expanded partnerships with the Expanded Programme on Immunization (EPI) community and health emergencies.
The informal event brought together a cross-section of stakeholders – partners, health actors, non-health actors, supporters, donors, Ministers of Health of endemic countries, WHO Regional Director for the Eastern Mediterranean, and Polio Oversight Board members – alluding to strengthened and systematic collaboration in areas of management, research and financing activities in the last mile.
Dr Zafar Mirza, Pakistan’s Minister of State,Ministry of National Health Services, Regulations and Coordination, took the stage and gave insight into country-level polio eradication efforts and the need for coordinated action with Afghanistan: “20 years ago, 30 000 children were paralyzed by polio in Pakistan. This year, 15 cases have been reported. While we have done a lot, it is clearly not enough. We are resolute in this conviction. We, together with Afghanistan, must make sure we eradicate polio for the sake of our children. Our science is complete, only our efforts are lacking. Along with the polio programme, the donors and the Afghan government, we will get to the finish line.”
Echoing similar sentiments, Dr Ferozuddin Feroz, Minister of Public Health of Afghanistan, said, “I would like to start by expressing thanks to all the partners for their support. As you know, Afghanistan has a very challenging context due to inaccessibility, refusals, gaps in campaign quality, low routine immunization coverage, and extensive cross-border movement. But, Afghanistan has made progress—five out of seven regions continue to maintain immunization activities. We view polio as a neutral issue and have developed a robust National Emergency Action Plan 2019. We appreciate the Polio Endgame Strategy 2019-2023. We believe coordination with Pakistan will help us deliver a polio-free world. We look forward to your continued technical and financial support to achieve the goal of polio eradication.”
Recognizing the long-standing commitment of the United Arab Emirates, a video was played showing the on-ground efforts of the Emirates Polio Campaign, working with communities and families in Pakistan in collaboration with the Global Polio Eradication Initiative and partners, and the Government of Pakistan. Thanks to the Emirates Polio Campaign, 71 million Pakistani children have been reached with 410 million doses of polio vaccine.
Dr Abdullahi Garba, Director for Planning, Research and Statistics, National Primary Healthcare Development Agency spoke on behalf of Professor Isaac F Adewole, Federal Minister of Health of Nigeria. Dr Garba harked back to the past as the GPEI plans for the future: “Nigeria started actively working to eradicate polio in 1988, at a time when we used to have up to a thousand cases every year. With all our innovation and efforts, I am pleased to inform you today that no wild polio case has been detected for the past 33 months. This feat was achieved through continuous efforts between the government, GPEI and partners, having diligent incidence reporting, reaching inaccessible children, and improving the quality of the polio surveillance immunization activities through strong oversight mechanisms in Nigeria. I know I also speak on behalf of all countries across Africa – we will achieve success.”
Rounding off the evening, Dr Tedros Adhanom Ghebreyesus, the World Health Organization Director-General and Chair of the GPEI Polio Oversight Board, took the stage to recount his first visit of the year to the polio endemic countries of Afghanistan and Pakistan, the progress made over decades, and the need to re-commit to the cause of ending polio. “Together with Regional Director Ahmed Al-Mandhari and Chris Elias of the Gates Foundation, we travelled to Pakistan and Afghanistan. We saw first-hand the commitments by both public and civil society leaders, which gave us a lot of confidence. The other thing that gave us confidence was seeing our brave health workers trudging through deep snow. And of course, our partners: Rotary, United Arab Emirates, CDC, UNICEF, the Bill & Melinda Gates Foundation and Gavi. The last 30 years have brought us to the threshold of being polio-free…(which) lay out the roadmap that is the Polio Endgame Strategy 2019-2023. The Ministers of Afghanistan and Pakistan have also assured us that they will continue to work together in their shared corridor to finish polio once and for all.”
In 1988, the World Health Assembly passed a resolution to globally eradicate poliovirus, in what was meant to be “an appropriate gift…from the twentieth to the twenty-first century.”
As the GPEI plans for the future and its final push to ‘finish the job,’ it is clear that political and financial efforts need to ramp up in this increasingly steep last mile. As he concluded, Dr Tedros thanked committed partners like United Arab Emirates: “Global progress to end polio would not be possible without partners like the UAE. I would like to thank His Highness Sheikh Mohamed bin Zayed Al Nahyan, Crown Prince of Abu Dhabi, and the UAE – a long-time supporter of the polio programme – for agreeing to host the GPEI pledging event this November at the Reaching the Last Mile Forum, a gathering of leaders from across the global health space held once every two years…let us join together to end polio.”
Participants of the Africa Regional Commission for the Certification of poliomyelitis eradication (ARCC) in Nairobi, Kenya, from 12-16 November 2018. WHO AFRO/2018
Efforts to end polio across the WHO African Region came under the microscope at a meeting of the Africa Regional Commission for the Certification of poliomyelitis eradication (ARCC) held in Nairobi, Kenya, from 12 – 16 November 2018.
Seven countries (Cameroon, Nigeria, Guinea-Bissau, the Central African Republic, South Sudan Equatorial Guinea and South Africa) made presentations to the ARCC on their efforts to eradicate polio, presenting evidence on their level of confidence that there is no wild polio in their borders, the strength of their surveillance systems, vaccination coverage, containment measures and outbreak preparedness. Kenya, the host country, alongside the Democratic Republic of the Congo and Namibia, presented updated reports on their efforts to maintain their wild poliovirus- free status.
Professor Rose Leke, Chair of the ARCC, speaking to the participants. WHO AFRO/2018
A total of 109 participants including partners of the Global Polio Eradication Initiative, non-governmental organisations and Health Ministries were in attendance to hear the reports.
The ARCC is an independent body appointed in 1998 by the WHO Regional Director for Africa to oversee the certification and containment processes in the region. It is the only body with the power to certify the Africa region free from wild polio. The African Regional Office and the Eastern Mediterranean Regional Office are the two WHO regions globally that remain to be certified free from wild poliovirus.
Professor Rose Leke, Chair of the ARCC, reflected on the importance of this meeting: “The rich, open and in-depth discussions held this week with each of the ten countries will allow these countries to strengthen ongoing efforts to further improve the quality of surveillance and routine immunization including in security compromised and hard to reach areas as well as in special populations such as nomads, refugees and internally displaced persons.”
Recommendations made
The ARCC, made up of 16 health experts, made recommendations to the ten countries. They noted with concern that outbreaks of circulating vaccine-derived poliovirus in the Democratic Republic of Congo, Kenya, Niger, Nigeria and Somalia were symptoms of low population immunity and varied quality vaccination campaigns. These countries were encouraged to conduct a high-quality outbreak response. Neighbouring countries were advised that they should assess the risk of spread or outbreaks within their borders. Low population immunity was identified as a significant concern, given the risk further emergences of vaccine-derived poliovirus strains.
Inaccessibility and insecurity were also flagged as a significant concern, with limits to the number of children who were being reached with polio vaccines and the coverage of surveillance efforts in affected areas. Countries were advised to scale up strategies that have proved in the past to be effective in the face of these challenges and to build relationships with civil society and humanitarian organisations who could provide immunization services.
Recommendations were made across the board to address chronic surveillance gaps, especially related to factors affecting the quality and transportation of stool samples reaching the laboratory for testing. The introduction of innovative technologies was commended, and a call was made for countries to expand their use, especially in inaccessible and hard-to-reach areas. Countries were also encouraged to accelerate their progress towards poliovirus containment.
In addition, all of the presenting countries received specific recommendations to support their efforts towards improving surveillance, immunization and containment in order to achieve a level that would give the ARCC the confidence needed to declare the region to have eradicated polio.
Dr Rudi Eggers, WHO Kenya Country Representative, said: “I commend all the countries on the efforts that have gone into achieving the results presented in their reports. It gives us hope that eradication is achievable in the midst of the unique challenges faced by all countries. We appeal to all the countries to fully implement all ARCC recommendations.”
Polio eradication efforts in Kenya
Dr Jackson Kioko, Director of Medical Services, the Kenyan Ministry of Health, said: “Kenya has worked hard to rid the country of wild poliovirus, and we will continue to do so until Africa and the world are certified polio-free.”
While Nigeria remains the only country in Africa to be endemic for wild poliovirus, responses are underway to stop outbreaks of circulating vaccine-derived poliovirus in the Democratic Republic of the Congo, Kenya, Niger and Somalia.
The circulating vaccine-derived poliovirus in Kenya was found in a sewage sample in Eastleigh, Nairobi, in March 2018, closely related to viruses found in Somalia. The Ministry Health, with the support of WHO, UNICEF and partners, has done several polio vaccination campaigns since then to ensure that every child’s immunity is fully built and no virus can infect them.
Chief Imman of Dutsen wai Sheck Zakaria Mohammed Sani sending message on RI and ANC during Eld-Kabir Prayer. UNICEF Nigeria
Malam Musa Abubakar was an ardent opponent of polio vaccination and other health services, not allowing his children to be immunized or his wives to receive antenatal care or other health services.
“I used to chase off immunization officers whenever they came to my door because I believed there was a hidden agenda behind it, and I was also uncomfortable allowing my wives to go to the hospital,” admitted Abubakar who hails from Zaria in Nigeria’s north-central Kaduna State.
Abubakar’s views changed, however, once Muslim clerics began to explain to the community the importance of allowing women and children to access health services and immunizations, along with the dire consequences of rejecting immunization services.
Delivering life-saving messages
Malam Ibrahim _Kaduan south RFP vaccinating a Child of NC house holdm at T-wada, Kaduna South LGA. UNICEF Nigeria
Religious, socio-cultural, and safety concerns are among the main barriers to polio vaccination and other health services in most of northern Nigeria.
United Nations Children’s Fund (UNICEF) has engaged 228 religious leaders in 11 northern Nigerian states, particularly in Muslim communities, to mobilize caregivers against social norms that prevent families from vaccinating their children. Muslim and Christian clerics deliver life-saving messages during sermons and other religious gatherings to dispel negative attitudes toward vaccinations and other health services.
Collaboration with religious leaders has not only supported polio eradication efforts but has also brought about further benefits in the fight against infant and maternal mortality through awareness campaigns.
“We have a duty to ensure people can live healthy lives”
Speaking at an annual meeting of 228 religious leaders held in Abuja in September 2018, Dr. Anis Siddique, UNICEF Chief of Communication for Development, described female and male religious leaders as game changers and encouraged them to create demand for immunization.
Sheik Abubakar Gumi, a renowned Muslim thought-leader and cleric, said that cooperation with religious leaders is creating positive change.
“Up until a few years ago, people in Muslim-majority communities stayed away from health centres, rejected polio vaccines and other routine immunizations even if they were brought to their doorstep due to misconceptions, suspicions, and socio-cultural norms,” explains Sheik Gumi. “But this changed with the engagement of religious leaders, who have succeeded in mobilizing people against behaviours that have put the lives of women and children at risk.”
Seeing respected religious scholars endorse immunization, others have also followed suit. Haruna, who leads Friday prayers at a mosque in Kaduna, speaks to over 1000 men every week about the importance of women and children accessing health services.
These collective efforts have brought about shifts in attitudes and knowledge as an average of 20 000 men who attend weekly Friday prayers across the mosques in northern Nigeria receive resounding messages on polio immunization and antenatal care-related health services.
“I used to be non-compliant but was convinced by Sheik Gumi about the dangers of rejecting immunization and other health services that are specifically provided to prevent women and children from dying of preventable diseases. As religious leaders we have a duty to ensure that all people can live healthy lives,” says Haruna.
In a rural village in Nigeria, a group of women knock on the door of new mother Hauwa Abubakar. She emerges from within, exhausted from the routine of feeding, sleeping, and caring for a little one. But she has extra reason than most to be tired.
A few months ago, she became mother to triplets, two baby girls and one baby boy.
The women visiting her are from her local community, but today they have come in their roles as polio vaccinators.
Realizing that they are there with vaccines, Hauwa picks up her young son, and carries him to another room. She closes the door, and returns to her daughters, ready to present them for their polio vaccinations.
The health workers ask Hauwa why she hid her son – he is just as vulnerable as his sisters, and the vaccine is the only way to keep him safe from polio paralysis.
“He is my only son,” she explains. “He will grow up and continue my family lineage. As for my girls, I’ll give them away to another family when they turn 18.”
“Boys or girls, your children all need polio immunization. Please don’t discriminate when it comes to matters of health,” says the lead health worker, as she puts two drops of polio vaccine into each of the girls’ mouths.
“You never know who your daughters will become one day, and you never know what disease you are protecting your son from.”
After a little more discussion, Hauwa is reassured. She fetches her son, and soon he too is protected from the virus.
Gender and polio eradication
Hauwa’s perspective is not unusual in communities where there is hesitation about the need to vaccinate. In communities where boys are more valued, and there is uncertainty about the need for vaccination, they may not be given the polio vaccine alongside their sisters. Sadly, this leaves them vulnerable to polio paralysis, whilst girls grow up protected from the virus.
Understanding that the world can only become polio-free if all children are vaccinated, the polio programme is developing a gender strategy which recognizes the way that gender impacts access to immunization, and also considers the valuable role of women health workers.
Dr Usman Adamu, the Incident Manager at the Nigerian National Emergency Operations Centre for Polio Eradication, explains how these things are related.
“All team members performing house-to-house for the polio campaign must be women. This is because we want to reach all eligible children with polio vaccines irrespective of whether children are inside or outside the house. Having a female team member makes it easy to reach these children in the household [where male vaccinators cannot enter]. ”
Polio workers are locally recruited, and women vaccinators often have a preexisting relationship with the mothers they visit with vaccines. This means that they are uniquely placed to answer questions and reassure them of the safety of the vaccine for boys and girls. With extra training, many women vaccinators also provide mothers with important information about other health interventions, including maternity health.
Keeping boys and girls safe
The GPEI gender strategy will help guide endemic countries like Nigeria to respond to gender related barriers to immunization. A first step has been the developing of several gender-sensitive indicators which country programmes use to track gender as a determinant of health.
The team lead of the WHO Immunization Cluster, Dr Fiona Braka, explains, “These gender-sensitive indicators measure the equal reach of girls and boys in vaccination campaigns, the doses of polio vaccine received by girls and boys, the timeliness of disease surveillance for girls and boys and women’s participation as front-line workers in polio-endemic countries.”
By recognizing the impact of gender on immunization, the polio programme can better deliver a vaccine to every baby.
For Hauwa’s triplets, the most important thing is that all three are well on their way to being protected from the virus.
“Please wait, I’ll soon be with you,” says Nasiru, the father of six children, as he disappears into his house in Gagi Makurdi settlement in Nigeria’s northwestern State of Sokoto.
Within minutes, Nasiru reappears, proudly displaying immunization cards with the record of the vaccines given to his youngest three children. It is unusual for fathers in this conservative part of Nigeria to readily know the whereabouts of these documents. Tending to children and ensuring that they stay healthy is usually a mother’s job.
“Take a look at the cards. My children Fidausi and Fatima have completed all their required immunization, whilst my youngest, Nana Asmaiu, is well on course to complete his,” he says.
Nasiru is a champion for immunization, but he wasn’t always so enthusiastic.
20 000 community mobilizers
It was Hauwa Ibrahim, a 46-year-old UNICEF-trained Volunteer Community Mobilizer, who persuaded Nasiru that the vaccine was safe and effective. She is part of a 20 000-strong network of community mobilizers who work across twelve Nigerian states like Sokoto, where some communities have been resistant to polio vaccination.
As recently as 2012, Nigeria used to account for half the world’s polio cases. Today, with help from women like Hauwa, no wild poliovirus has been detected in the country since August 2016. There are still many immunity gaps in Nigeria – as underlined by an outbreak of vaccine-derived virus currently ongoing in the country – but in the villages where VCMs like her work, these gaps are beginning to close.
Using a simple register, Hauwa goes house to house in Gagi Makurdi to record all children below the age of five, as well as women who are pregnant. It is the same register that Hauwa used to track the pregnancies of Nasiru’s wife – Zara’u – and she now uses it to find out who manages the routine immunization schedules of the three youngest children in the household.
Strengthening routine immunization
This forms part of the polio programme’s work in Nigeria to strengthening routine immunization, building on the infrastructure developed to eradicate the virus.
Upon her first visit, Hauwa was determined to convince Nasiru that vaccination against polio and other diseases is important – and that he should take the children to the health facility.
“My culture does not allow a wife to go outside of the compound, so when Hauwa insisted that we take our children to the health facility for vaccines, I had no way but to go myself. Else, Hauwa would not give up,” Nasiru explains. Whilst he travels with his children, Zara’u takes care of their older siblings at home.
By recruiting locally influential women like Hauwa from communities where some parents are vaccine-hesitant, and training them to be advocates for child health, vaccination rates are improved throughout their neighbourhoods. In some areas, more than 99% of parents now accept the polio vaccine for their child.
“Hauwa resides in this settlement and I trust her; I trust that the advice she is giving is in the best interest of my children,” says Nasiru.
He also notes, however, that he is often the only man at the health facility.
Engaging all fathers
Hauwa hopes that by encouraging more fathers to take on the parental responsibility of completing their children’s routine immunization schedule, immunization coverage will increase across Sokoto. Greater vaccine acceptance and awareness means that children are more likely to receive a life-saving polio vaccine, and other vaccines, whether through routine immunization or through door-to-door vaccination.
Already, the trust that she has built amongst parents in Gagi Makurdi has helped surmount many of the barriers that deny children immunization and other health services. In Nasiru and Zara’u’s compound, nearly all children are now protected against polio and other vaccine-preventable diseases.
Only their baby, Nana Asmaiu, has yet to have all his vaccinations – and Hauwa will soon visit his household to support Nasiru and Zara’u, and ensure he gets them.
Nine hours away from the nearest large town, Dr Adele Daleke Lisi Aluma speaks to Robert, who manages a small health clinic on an island in the Lake Chad Basin. With paperwork spread around them, she listens carefully he responds to each question: Can you tell me how to recognise the symptoms of a potential polio case? Can you show me the records of any measles cases since I last visited?
In the past, she would be writing down details of the disease surveillance system in this village in a notebook, spending time later typing up her notes, and emailing them to a central database. Today, thanks to the introduction of an electronic surveillance approach for active surveillance and monitoring of disease outbreaks, she inputs Robert’s answers directly into an app, allowing for quick, accurate, and up-to-date data collection.
Hundreds of kilometres away in Nigeria, on the other side of the basin, surveillance officer Dr Namadi Lawal also feels the difference that innovative application-based technology has made to operations. For years, his employer, the National Primary Health Care Development Agency, depended on paper-based recording methods.
When the World Health Organization introduced the electronic surveillance (e-Surve) approach, Dr Namadi discovered he was receiving far more accurate information in real time, making his work to defeat the poliovirus more efficient.
“e-Surve is such a wonderful innovation. I can only imagine how much more accurate data I would have collected in a fast and effective manner if I had adopted this approach long time ago,” he says.
The e-Surve approach involves the use of a smartphone application to ensure that health workers know what symptoms they should be looking for and how to report suspected cases of vaccine-preventable disease.
After using the application to guide their conversations with health workers, disease surveillance and notification officers send the results of the questionnaire to a central database, where the data can be analysed and sorted by health district.
This is one way to keep track of an outbreak response that covers areas of five different countries, all with their own unique health challenges.
“This is remarkable progress as it shows where we can actually reach for surveillance”, said Dr Isaac Adewole, Nigeria’s Minister of Health, as he was presented with a dashboard of e-Surve during the recent opening ceremony of the African Regional Certification Commission in Nigeria.
New technology helps to reduce outbreak risk
This innovation is particularly important as when cases of disease are not properly reported, an outbreak can be in full swing before a country even realises that there is a problem.
Active disease surveillance, where officers physically go out to communities to speak to health staff and parents, is proven to increase case detection rates. There are hundreds of these frontline workers spread out across the Lake Chad Basin, each conducting multiple visits every month. Before mobile technology, the outcomes of these visits were cumbersome to track, time consuming to catalogue, and difficult to analyse for a prompt response.
Real-time reporting stems the spread of diseases
With e-Surve, governments and partners in the polio programme and other health programmes can easily see trends, track data, and take action. This encourages a preventive approach to disease outbreaks rather than a reactive one.
In Nigeria, as of May 2018, about 18 840 active surveillance visits to health facilities had been made using e-Surve technology: as a result, over 3000 suspected cases of vaccine-preventable diseases – previously unreported from health facilities – were identified and investigated.
Strong support from government
Behind the new technology stands commitment from governments, communities, and partners to close the polio outbreak response. Dr. Sume Gerald at the WHO Nigeria office, states that “e-Surveillance in Nigeria is government-led and driven, supported by WHO.”
Through innovation, determination, and commitment at all levels, those working to end polio are getting ever closer to their goal.
Three-year-old Ibrahim wouldn’t stop crying. Suffering from ringworm, a fungal infection, his leg had become badly infected. Left untreated, he risked developing fever and scarring wounds.
For Ali Musa, his father, it was hard to know where to turn for help. Where he lives, in the nomadic community of Daurawa Shazagi in the Nigerian state of Jigawa, there is little access to professional medical treatment.
From his home, it would take Ali a full day to trek to the nearest primary health centre. He does not recall the last time anyone in his community made this “practically unthinkable” journey.
Reaching all children with vaccines
“But when I heard in the market that a medical team was coming to us to treat sick people, especially women and children, I went with the hope to at least get him some relief from the pain,” Ali recalls.
There, Ali met members of the mobile health teams supported by the UNICEF Hard-to-Reach (HTR) project – funded by the Government of Canada’s Department of Foreign Affairs, Trade and Development. These teams are helping to ensure that children receive polio vaccinations, whilst also providing basic health services – including medications to fight infections like ringworm – in hard-to-reach areas of Nigeria.
The teams vaccinate against measles, meningitis and other diseases, and provide vitamin A supplements and deworming tablets for children. They also carry out health promotion activities, teaching communities about important practices such as exclusive breastfeeding. During each clinic, members of the HTR team give two drops of polio vaccine to every child, ensuring that all are protected from the virus.
At the end of their visit, the team pack up the clinic, and travel home, taking hours to cross difficult terrain by foot, boat and motorbike.
2390 children vaccinated
The HTR project aims to reduce the immunity gap among children living in Nigeria. Since 2016, when cases of wild poliovirus last were detected in the country, determination and commitment have helped to strengthen eradication efforts, but many states still face an uphill task to increase historically low routine immunization rates. This is especially the case in rural areas, where there are few services, and communities have to travel far to the nearest health clinic.
So far in 2018, the project has reached thousands of previously unvaccinated children with the life-saving polio vaccine, including 2390 children in Ibrahim’s state, Jigawa.
“Why should I let anything stop me?”
Salamatu Kabir, who leads a HTR team assigned to take immunization and basic health care services across Jigawa, says “I look at it this way. If people from outside can come all the way to bring the hard-to-reach project to my country, why should I let anything stop me from delivering it to my own people who are most in need?”
A retired health worker, she says that she doesn’t think twice about the many hurdles that she will have to overcome to reach children in communities like Ali and Ibrahim’s.
Far more of a concern is planning meals for her four children whilst she is away, and packing all the equipment she will need for the journey. Experience over the years has taught her what items to add to her bag besides vaccines. She always carries an umbrella, an extra pair of clothes, insect repellant and depending on the season, either an additional pair of sandals or, most often, rain boots.
Salamatu asserts that for the team members, “visiting the settlements to administer health care is something we have come to love and look forward to”.
When the team finally does arrive at their destination they are greeted by an expectant community. Salamatu is motivated by the direct impact her work has on the lives of others.
Little Ibrahim is one of those to benefit. After treatment from the team, his condition improved quickly. His father Ali has since become a volunteer for the HTR project, and an avid advocate within his community for medical care.
“I will do my best to ensure every child in my village benefits from the help that is coming from far,” he says.
Binta Tijjani works to eradicate polio in her native Kano state of Nigeria. She is one of the over 360 000 frontline workers dedicated to ending polio in her country, the vast majority of whom are women. Nigeria is one of only three countries in the world yet to stop poliovirus circulation, together with Afghanistan and Pakistan.
Binta has worked in polio eradication for over 14 years. Starting as a house-to-house vaccination recorder, she was soon promoted to the role of polio campaign supervisor and now works as an independent polio campaign monitor.
“My biggest strength is my ability to work closely with our teams to ensure we reach every last child with vaccines, and advising teams so they can ask the right questions and raise important issues in each household they visit,” Binta says.
Working with the polio programme often opens up other opportunities for women to enter the workforce and utilize their skills to contribute to their communities, leading to positive investments beyond polio eradication.
“My work with the polio programme has enabled me to buy land and take care of my children’s school fees and our household needs. Currently I’ve enrolled in a course to get a certificate in catering. My dream is one day to open a restaurant,” Binta says.
Similar to Binta, Halima Waziri has been serving the polio eradication cause in different roles since 2005. Currently Halima works as a lot quality assurance sampling interpreter in Kano state, assessing the quality of vaccination coverage after immunization campaigns in her area.
“I am most proud of engaging in many productive dialogues about polio vaccination in remote and hard-to-reach areas and high-risk communities in Nigeria. This has helped me to improve my interpersonal communication skills and given me confidence in public speaking and influencing people,” Halima says.
With the money she has earned as a polio worker, Halima has opened a medicine store where she sells medicines and also acts as a community informant and focal point for disease surveillance.
Nigeria was on the brink of eradicating polio when a new wild poliovirus case was reported in 2016 after two years without any confirmed cases. Low overall routine immunization coverage is a key stumbling block to eradication, combined with ongoing violent conflict in the northeast where over 100 000 children remain inaccessible for vaccination teams.
Nigeria continues to implement an emergency response to vaccinate all children under the age of 5 to ensure they are immunized and protected, including implementing vaccination campaigns whenever security permits, vaccinating children at markets and cross-border points, and conducting active outreach to internally displaced people.
Without the critical participation of women as vaccinators, surveillance officers and social mobilizers, Nigeria would not be as close to eradicating polio as it is today. The latest nationwide immunization campaign, synchronized with countries in the Lake Chad basin, aimed to reach over 30 million children in Nigeria in April.
No wild poliovirus cases have been reported in 2017 or 2018. Binta and Halima, together with an army of frontline workers, are determined to keep it this way and secure a polio-free future for Nigeria.
 Known by colleagues and friends as Emeka, 45, was a valued member of the WHO workforce for the last ten years, supporting immunization, polio eradication, and Ebola outbreak response in the African and Eastern Mediterranean regions.
Known by colleagues and friends as Emeka, 45, was a valued member of the WHO workforce for the last ten years, supporting immunization, polio eradication, and Ebola outbreak response in the African and Eastern Mediterranean regions.