Polio transition involves repurposing polio assets – knowledge, network and infrastructure – to strengthen the broader public health functions of a country within the overall context of strengthening the national health system. These wider functions include immunization, vaccine-preventable diseases surveillance, and emergency preparedness and response.
To safeguard polio essential functions through sustainable resources, it is crucial to achieve the full transition by shifting from external to domestic financing. In turn, successful polio transition and the integration and maintenance of polio assets to strengthen routine immunization, disease surveillance and outbreak response have social and economic benefits and offer a very high return on investment.
Efforts to protect children from polio take place all over the world, in cities, in villages, at border checkpoints, and amongst some of the most difficult-to-access communities on earth. Vaccinators make it their job to immunize every child, everywhere.
In places where families are displaced and on the move due to conflict, it is especially important to ensure high population immunity, to protect all children and to prevent virus spread. In Iraq last month, vaccinators undertook a five-day campaign in five camps for internally displaced people around Erbil, in the north of the country, as part of the first spring Subnational Polio campaign targeting 1.6 million children in the high risk areas of Iraq (mainly in internally displaced person camps, and newly accessible areas).
Iraq has not had a case of indigenous wild poliovirus since 2000. However, due to the drastic drop in immunity in the country after years of conflict, two children were paralyzed when wild poliovirus was imported in 2014.
Poliovirus spreads from person to person, transmitted through populations. Last year, there were 74 cases of polio in Raqqa and Deir ez-Zor governorates in Syria. Over the border in Iraq, children in Mosul and Anbar are deemed to be at high risk of being infected because of the history of regular movement of armed groups between the two countries. Violence has caused many families to leave their homes – potentially carrying the virus with them as they travel to internally displaced persons camps and other destinations.
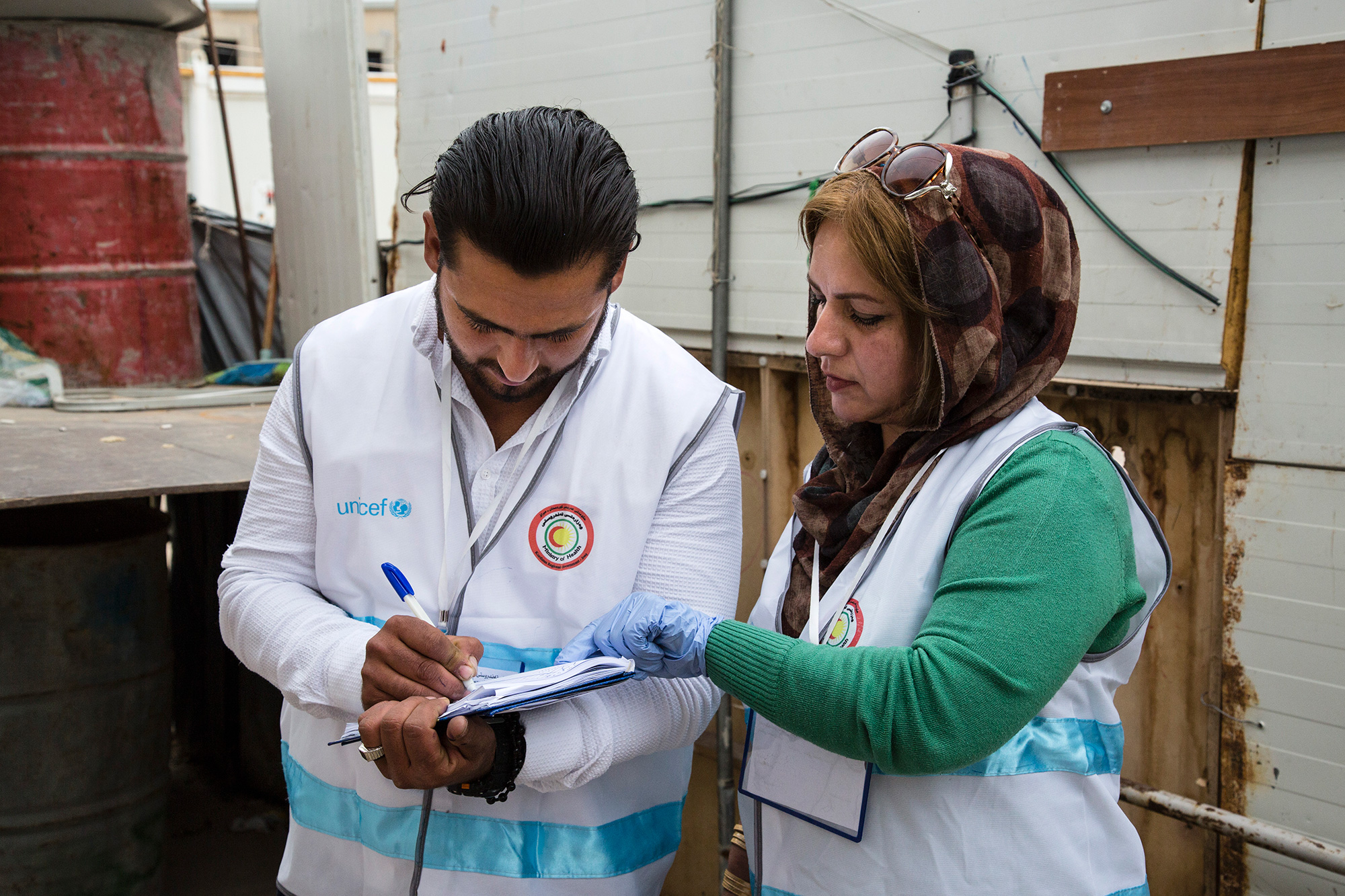
Baharka camp, one of the five internally displaced persons camps near Erbil, is where many families from Mosul, Anbar, and other areas currently reside. During the polio vaccination campaign, male and female vaccinators walked tent-to-tent to deliver vaccine to all children under the age of five. Their aim was to ensure whole-camp immunity by finding and protecting every child.
After visiting a household, the vaccinators marked on wood, stone and canvas how many children had received vaccine, along with information about any vaccine refusals. Over the course of the campaign, vaccinators aimed to reach 4203 children.
As well as twice-yearly vaccination campaigns, health workers in the Erbil camps look for signs of Acute Flaccid Paralysis (AFP) amongst children living there, which is one of the most common indicators of polio. Any suspected cases are recorded, and investigated through the poliovirus surveillance network. Since surveillance began in the camps, thirty AFP cases have been discovered and investigated for signs of the virus.
“We conduct continuous monitoring,” said WHO Polio Eradication Officer Dr Rebaz Lak. “If any child displays weakness of the limbs, the doctor must notify health authorities.”
Since 2014, more than five million civilians have fled their homes inside Iraq. At the same time, families are returning to places where instability has lessened. As many as two million displaced Iraqis are likely to return home this year, which means children will be on the move once more. This makes the vaccination of every child even more important – allowing them to travel safely, and be protected from virus when they reach their destination.
Some families choose to go home, but keep a safe place to flee to should violence return. Since Baharka camp opened, a number of families have travelled back to Mosul, but have maintained their displaced person status and a caravan in the camp. The World Health Organization carefully monitors the names and caravan numbers of the children in these groups, to ensure that vaccinators visit them whenever there is a campaign. Once vaccinated, each child has their little finger stained purple – an easy way to prevent children being missed.
Alongside the children protected in Baharka camp, the Global Polio Eradication Initiative partners vaccinate over 400 million children every year. Efforts to eradicate polio also help to fight other diseases at the same time, whilst the valuable polio eradication infrastructure, data and tools can help to strengthen the health systems of conflict-affected countries.
Thanks to the devotion of vaccinators and health workers, the displaced children of Mosul and Anbar are protected together from the virus. When they return home, they won’t have missed out on a valuable health intervention – allowing them to lead healthier, polio-free lives in the future.
Amidst conflict and humanitarian crisis in Syria, health workers are battling to end the current polio outbreak. Since the World Health Organization announced the outbreak on 8 June 2017, 70 cases have been confirmed, with 67 in Deir Ez-Zor governorate, two in Raqqa and one in Homs.
Vaccinating children
WHO and UNICEF are supporting the Government of Syria and local authorities to end the outbreak. Two mass vaccination campaigns have taken place, thanks to dedicated health care workers on the ground, striving to reach resident, refugee and internally displaced children. Despite the challenges of holding vaccination campaigns in a conflict zone and effectively reaching displaced populations from infected areas, more than 255,000 have been vaccinated in Deir Ez-Zor, and more than 140,000 in Raqqa.
Contingency plans for an additional vaccination campaign are being put in place to reach children under the age of five with monovalent oral polio vaccine type 2 in the infected zones and areas hosting high risk populations, particularly recently displaced families from Deir Ez-Zor.
Two different vaccines are being used to ensure that population immunity against polio is rapidly increased. The monovalent oral polio vaccine type 2 is being used to rapidly increase immunity against type 2 polio. To boost immunity against type 2 and also provide protection against types 1 and 3, the inactivated poliovirus vaccine is also being provided to children aged between 2 and 23 months in high risk areas.
Preventing spread of polio
While all hands are on deck to stop polio, outbreak response teams are also working hard and adapting complementary strategies such as vaccination at transit points and registration centres for internally displaced persons from infected zones, to prevent spread of the virus to other parts of the country. The inactivated poliovirus vaccine is being used strategically in high risk areas, especially where there are high numbers of internally displaced families.
In order to reduce the threat of polio spreading to the countries surrounding Syria, vaccination activities have been carried out in Iraq, Lebanon and Turkey. These activities are aiming to reach both Syrian children and those from local communities to limit the possibility for the virus to spread across international borders.
Searching for the virus
Knowing where the virus is at all times is crucial to stop the outbreak. Surveillance is ongoing across the country, with doctors, community members and vaccinators on the alert for any child with potential symptoms of polio. The surveillance system is operating well, despite the challenges of transporting stool samples from children with symptoms to laboratories for testing.
Plans are also in place to begin environmental surveillance in Syria by the end of the year. This will enable laboratories to identify the presence of polio in sewerage to provide early warning.
The information from disease surveillance being used to inform where and when vaccination campaigns need to take place.
Vaccine derived polio
The current outbreak in Syria is caused by circulating vaccine derived poliovirus type 2, a very rare virus that can occur when population immunity against polio is very low. In Syria, conflict and insecurity have compromised community access to immunization services, which has allowed the weakened virus in the oral polio vaccine to spread between under-immunized individuals and, over a long period of time, mutate into a virulent form that can cause paralysis. The only way to stop transmission of vaccine-derived poliovirus is with an immunization response, the same as with any outbreak of wild polio. With high levels of population immunity, the virus will no longer be able to survive and the outbreak will come to a close.
Amman, 7 April 2014– Polio vaccination campaigns have commenced in Syria, Iraq and Egypt, aiming to reach more than 20 million children over five days.
For Iraq, this will be the first nationwide vaccination campaign since a case of polio was confirmed by the Ministry of Health on 30 March in a six-month-old boy from Rusafa, northern Baghdad.
“The recent detection of a polio case in Iraq after a 14-year absence is a reminder of the risk currently facing children throughout the region,” said Maria Calivis, UNICEF Regional Director for the Middle East and North Africa. “It is now even more imperative to boost routine immunisations to reach every child multiple times and do whatever we can to vaccinate children we could not reach in previous rounds. That’s the only way we will prevent this outbreak from spreading further.”
The current vaccination rounds are part of a comprehensive response to the announcement, in October 2013, that wild poliovirus of Pakistani origin had found its way to Syria. In recognition of the risk of further international spread, the governments of seven countries across the Middle East, with the assistance of local non-governmental organizations, civil society groups and UN agencies, are endeavouring to reach 22 million children multiple times with polio vaccine. Since October 2013, 25 polio vaccination campaigns were completed across the region, including five rounds in Syria and six in Iraq.
The numbers of children being vaccinated in each round is rising; however, the outbreak response is yet to reach especially vulnerable groups such as children who are on the move fleeing violence from Syria or those living in the midst of active conflict.
“Midway into the implementation of this outbreak response plan, we’re reaching the vast majority of children across the Middle East,” said Chris Maher, WHO Manager for Polio Eradication and Emergency Support. “In the second phase of the outbreak response we must work with local partners to reach the hardest-to-reach – those pockets of children who continue to miss out, especially in Syria’s besieged and conflict areas and in remote areas of Iraq. We won’t stop until we reach them.”
Health teams in Lebanon and Turkey will also join the campaign on 10 and 18 April.