Compared to the busy streets of Hargeisa, Somaliland, just 20 kilometres outside of the city are broad stretches of barren land—home to the nomads. Nomadism is part of Somalia’s culture, and there are thousands of families throughout the country who lead pastoral lifestyles, raising livestock and moving their animals and families as the seasons change. Their frequent movement means that children are not always nearby a health clinic to receive their scheduled vaccinations on time. Such disruption or delay in receiving vaccines can result in low or no protection against common childhood infections.
If children are not immunized against polio, they risk contracting the virus and developing paralysis. They also risk passing polioviruses to other under-immunized children. But the polio eradication teams are committed to reach every last child with polio vaccine notwithstanding challenging terrains.
Look through the lives of polio vaccinators in Somaliland on the third day of the vaccination campaign activities as part of the larger efforts to reach over 1.1 million children with the oral polio vaccine.

It’s 7am, and a late August dawn is stretching across a broad, sparsely populated landscape. At the side of the dirt track road, a man herds a group of camels to their grazing land for the day.
Today, their focus is the children living among nomadic communities.

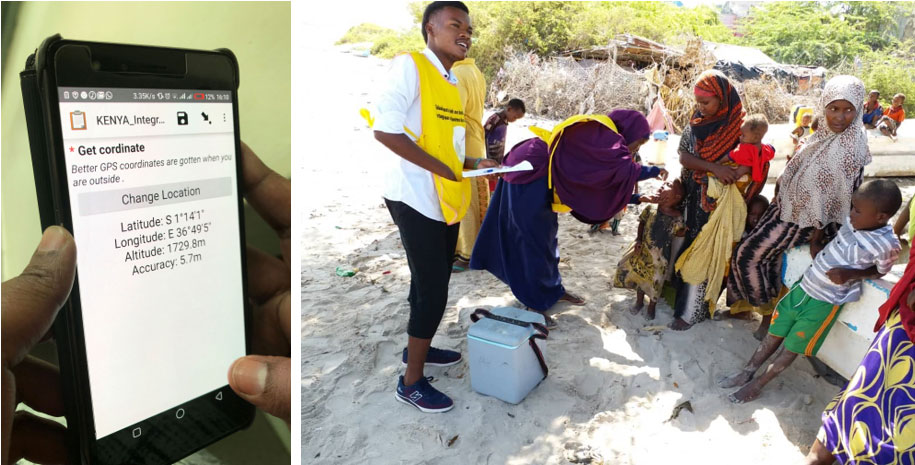
Parking up amongst stones and tree roots, with arid scrub-land stretching away behind the 4x4, the vaccination team pull on their Somalia Polio Programme vests, which identify them as health workers, and retrieve their vaccine cold box from the back of the car.
The team is tired from the early start, but excited to provide vaccine to these communities.

One of the most rewarding parts of the job is reaching children who are yet to have their first polio vaccine dose.
In one of the first homes visited, the team finds a tiny newborn wrapped in a swaddling-cloth.

Abdirisaq Nimcan Mohamed is just two days old. Vaccinator Suad Hashi Handule gently squeezes his cheeks so that he opens his mouth for the vaccine.
Two drops later, and this little one is on his way to being fully protected against the poliovirus.

Tiny newborn fingers are too small to mark with indelible ink to show that the child has received a vaccine today, so instead, Suad stains Abdirisaq’s big toe before he is tucked back into his warm blankets.
Suad discusses with the family that there are other vaccines that are essential for Abdirisaq to receive to stay well. She encourages his parents to take him to the nearest health clinic when the time comes for his next scheduled doses.
When he is 14 weeks old, he should receive the injectable polio vaccine, which will ensure he is fully protected against all polio virus strains.

As they vaccinate, the health workers are also busy greeting the local community and strengthening awareness of the importance of vaccination.
Being willing to have a discussion about the vaccine helps to build trust with families and gives health workers an insight into the lives of the children they are vaccinating.

By 11am, the teams have vaccinated every child under age five in this nomadic community.
Along the way, they’ve attracted interest from excited children, encountered curious goats and camels, and increased awareness of the importance of polio vaccination for every child.

The next time polio vaccinators encounter this community, they might be residing in a completely different spot.
Close community relationships help the Somalia polio programme know where nomadic groups are moving to, meaning that they can be visited again when the next vaccination campaign happens.

This campaign was the third round to take place as part of the latest stage of polio outbreak response in reaction to virus detected in the north of Somalia. The next campaign, using a different vaccine, is scheduled for this coming autumn.
Back in the car, the vaccinators set off for their next destination, driving slowly on the bumpy roads.
They are dedicated to delivering vaccines to all children, no matter where they live.