Community Sensitization for the Whole Family Approach (WFA) activities in Abuja, Nigeria. Photo: Vaccine Network for Disease Control (VNDC)
According to the United Nations, a civil society organization (CSO) is any non-profit, voluntary citizens’ group which is organized on a local, national, or international level. CSOs have a vital role to play in the control of infectious diseases. Some CSOs play an advocacy role to sustain commitments of governments, communities, and donors, some support implementation of program activities, and some do both.
The UN Foundation’s new report, “Leveraging CSO Contributions to Advance Polio Transition and Integration Efforts in the African Region” outlines specific areas where CSO support can be of value for polio transition and integration. In particular, this report describes the initiatives implemented by four CSOs supported by the UN Foundation to enhance polio transition and integration efforts in the Democratic Republic of the Congo (DRC), Ethiopia, Nigeria, and South Sudan.
STATUS OF POLIO IN THE AFRICAN REGION
The African region was declared free of wild poliovirus (WPV) in August 2020. This incredible achievement was a result of decades of work by a coalition of international health bodies, national and local governments, civil society and community volunteers. Notwithstanding this significant milestone, the African Region is still experiencing outbreaks of the non-wild variant of poliovirus, known as circulating vaccine-derived poliovirus (cVDPV) in 25 countries. Furthermore, in 2022, WPV importations were reported in two countries that had been polio-free for over three decades, Malawi and Mozambique. These detections highlight that until all forms of polio are eradicated everywhere, the risk of importation remains a constant threat. This further emphasizes the importance of maintaining the Global Polio Eradication Initiative (GPEI) infrastructure in order to both achieve and maintain a polio-free world.
In this two-part video series, we chat with Dr Ananda Bandyopadhyay, Deputy Director of Polio Technology, Research & Analytics, BMGF, about the new tool in GPEI’s kit to combat cVDPV2: novel oral polio vaccine type 2 (nOPV2).
GENEVA, 26 April 2022
Today, the Global Polio Eradication Initiative (GPEI) announced that it is seeking new commitments to fund its 2022-2026 Strategy at a virtual event to launch its investment case. The strategy, if fully funded, will see the vaccination of 370 million children annually for the next five years and the continuation of global surveillance activities for polio and other diseases in 50 countries.
During the virtual launch, the Government of Germany, which holds the G7 presidency in 2022, announced that the country will co-host the pledging moment for the GPEI Strategy during the 2022 World Health Summit in October.
“A strong and fully funded polio programme will benefit health systems around the world. That is why it is so crucial that all stakeholders now commit to ensuring that the new eradication strategy can be implemented in full,” said Niels Annen, Parliamentary State Secretary to the Federal Minister for Economic Cooperation and Development, Germany. “The polio pledging moment at the World Health Summit this October is a critical opportunity for donors and partners to reiterate their support for a polio-free world. We can only succeed if we make polio eradication our shared priority.”
Wild poliovirus cases are at a historic low and the disease is endemic in just Pakistan and Afghanistan, presenting a unique opportunity to interrupt transmission. However, recent developments, due in part to impacts of the COVID-19 pandemic, underscore the fragility of this progress. In February 2022, Malawi confirmed its first case of wild polio in three decades and the first on the African continent since 2016, linked to virus originating in Pakistan, and in April 2022 Pakistan recorded its first wild polio case since January 2021. Meanwhile, outbreaks of cVDPV, variants of the poliovirus that can emerge in under-immunized communities, were recently detected in Israel and Ukraine and circulate in several countries in Africa and Asia.
The investment case outlines new modelling that shows achieving eradication could save an estimated US $33.1 billion this century, compared to the price of controlling polio outbreaks. At the launch event, GPEI leaders and polio-affected countries urged renewed political and financial support to end polio and protect children and future generations from the paralysis it causes.
“Despite enormous progress, polio still paralyses far too many children around the world – and even one child is too many,” said UNICEF Executive Director Catherine Russell. “We simply cannot allow another child to suffer from this devastating disease – not when we know how to prevent it. Not when we are so close. We must do whatever it takes to finish the fight – and achieve a polio-free world for every child.”
“The re-emergence of polio in Malawi after three decades was a tragic reminder that until polio is wiped off the face of the earth, it can spread globally and harm children anywhere. I urge all countries to unite behind the Global Polio Eradication Initiative and ensure it has the support and resources it needs to end polio for everyone everywhere,” said Hon. Khumbize Kandodo Chiponda MP, Minister of Health, Malawi.
The new eradication strategy centres on integrating polio activities with other essential health programs in affected countries, better reaching children in the highest risk communities who have never been vaccinated, andstrengthening engagement with local leaders and influencers to build trust and vaccine acceptance.
“The children of Pakistan and Afghanistan deserve to live a life free of an incurable, paralyzing disease. With continued global support, we can make polio a disease of the past,” said Dr Shahzad Baig, National Coordinator, Pakistan Polio Eradication Programme. “The polio programme is also working to increase overall health equity in the highest-risk communities by addressing area needs holistically, including by strengthening routine immunization, improving health facilities, and organizing health camps.”
The investment case outlines how support for eradication efforts will enable essential health services in under-served communities and strengthen the world’s defences against future health threats.
Since 2020, GPEI infrastructure and staff have provided critical support to governments as they respond to the COVID-19 pandemic, including by promoting COVID-safe practices, leveraging polio surveillance and lab networks to detect the virus, and assisting COVID-19 vaccination efforts through health worker trainings, community mobilization, data management and other activities.
“The global effort to consign polio to the history books will not only help to spare future generations from this devastating disease, but serve to strengthen health systems and health security,” said Dr. Tedros Adhanom Ghebreyesus, WHO Director-General.
Additional quotes from the GPEI Investment Case:
“We have the knowledge and tools to wipe polio off the face of the earth. GPEI needs the resources to take us the last mile to eradicating this awful disease. Investing in GPEI will also help us detect and respond to other health emergencies. We can’t waver now. Let’s all take this opportunity to fully support GPEI, and create a world in which no child is paralyzed by polio ever again,” said Bill Gates, Co-chair, Bill & Melinda Gates Foundation.
“An investment in polio eradication goes further than fighting one disease. It is the ultimate investment in both equity and sustainability – it is for everyone and forever. An important component of GPEI’s Strategy focuses on integrating the planning and coordination of polio activities and essential health services to reach zero-dose children who have never been immunized with routine vaccines, therefore contributing to the goals of the Immunization Agenda 2030.” said Seth Berkley, Chief Executive Officer, Gavi, the Vaccine Alliance.
“Twenty million people are walking today because of polio vaccination, and we have learned, improved and innovated along the way. We are stronger and more resilient as we enter the last lap of this marathon to protect all future generations of the world’s children from polio. Please join us; with our will and our collective resources, we can seize the unprecedented opportunity to cross the finish line that lies before us,” said Mike McGovern, Chair, International PolioPlus Committee, Rotary International.
Sabrina Sidhu
UNICEF New York
Email: ssidhu@unicef.org Tel: +19174761537
April 2022 – Convening this month in Geneva, Switzerland, the Strategic Advisory Group of Experts on immunization (SAGE), the global advisory body to the World Health Organization (WHO) on all things immunization, urged concerted action to finish wild polioviruses once and for all.
The group, reviewing the global wild poliovirus epidemiology, highlighted the unique opportunity, given current record low levels of this strain. At the same time, it noted the continuing risks, highlighted in particular by detection of wild poliovirus in Malawi in February, linked to wild poliovirus originating in Pakistan.
On circulating vaccine-derived poliovirus (cVDPV) outbreaks, SAGE expressed concern at continuing transmission, in particular in Nigeria which now accounts for close to 90% of all global cVDPV type 2 cases, as well as the situation in Ukraine, and its disruption to health services, urging for strengthening of immunization and surveillance across Europe. It also noted the recent detection of cVDPV type 3 in Israel in children, and in environmental samples in occupied Palestinian territories, and urged high-quality vaccination activities and strengthened surveillance.
Preparing for the post-certification era, the group underscored the importance of global cessation of all live, attenuated oral polio vaccine (OPV) use from routine immunization, planned one year after global certification of wild poliovirus eradication. To ensure appropriate planning, coordination and implementation, the group endorsed the establishment of an ‘OPV Cessation Team’, to consist of wider-than-GPEI stakeholder participation and ensure leadership on all aspects of OPV cessation.
SAGE will continue to review available evidence and best practices on a broad range of GPEI-related programmatic interventions, including as relevant the increasing role of inactivated polio vaccine (IPV), including in outbreak response and effects of novel oral polio vaccine type 2 (nOPV2), as part of global efforts to secure a lasting world free of all forms of poliovirus.
Dr Pascal Mkanda, Director for the Polio Eradication Programme in the World Health Organization’s Regional Office for Africa (AFRO), also famously known as our ‘villager in polio’, is this month (February 2022) entering a well-deserved retirement. Pascal’s contribution over the years to polio eradication in Africa, and indeed broader immunization, is second to none.
Under Pascal’s stewardship and leadership, wild polioviruses were successfully eradicated from the continent, the polio infrastructure integrated into broader public health efforts, new technologies and innovations for reaching the most marginalized children established and new vaccines successfully rolled-out. His expertise, knowledge, dedication, zeal, and passion to work and more importantly his mentorship to fellow colleagues and health workers to alleviate the lives of vulnerable children across the continent, will be sorely missed.
“I have worked with Pascal for close to 7 years, and during that time, I have witnessed first-hand Pascal’s dedication, and what he often refers to as ‘tough’ decision making, which we owe to the successes we have seen in the polio program” said Dr Matshidiso Moeti, WHO Regional Director for Africa.” My first interaction with Pascal was during the first meeting for Program Managers in the region, in Johannesburg, South Africa, in 2016. During this meeting Pascal expressed very passionately that the only way we can get results in Polio is by holding everyone accountable. To use his words, global health, very much like soccer, requires a coach to put his best players on the field. Throughout the continent, children are healthier and better protected from infectious diseases, most notably of course from polio, thanks to the tremendous efforts and tireless work of Pascal. This continent owes a huge debt of gratitude to Dr. Mkanda. On behalf of all mothers of Africa, I can simply only say one thing: Thank you, Pascal!”
“Rotary and Rotary members across Africa have been at the forefront in the fight against polio since President Nelson Mandela shouted his rallying call in 1996 to ‘Kick Polio Out of Africa’,” according to Dr Tunji Funsho, Chair of Rotary’s Nigeria National PolioPlus Committee and one of TIME Magazine’s 100 Most Influential People in 2020. “We went from 75,000 children paralyzed each year, all over Africa in 1996, to Zero wild polio cases since 2016. An unparalleled public health achievement, which could not have happened without Pascal’s leadership, engagement, and expertise. On behalf of Rotary members across Africa, Pascal – thank you so much for everything that you have done. We all wish you a more than well-deserved retirement.”
“I can only echo what others have already said,” commented Professor Rose Leke, Chair of the African Regional Certification Commission, which independently certified Africa as wild poliovirus free in 2020. “It was my great honour, and together with my fellow Commission Members, to certify our continent free of all wild polioviruses. Dr Mkanda and his team across the continent were absolutely instrumental in this. As Director of Polio in the Region, he exhibited great leadership. He and his team helped us verify the absence of wild poliovirus, even from the most inaccessible and remote areas of Africa. They helped ensure that children everywhere, no matter where they lived, were reached with the life-saving polio vaccine. Dr Mkanda demonstrated truly the best of Africa. All I can say is a tremendous ‘thank you’ to him and his team. I wish him well in all his future endeavours.”
Dr Mkanda’s career started from humble beginnings in a small and remote village, Chintheche in northern Malawi, with virtually no infrastructure. Pascal, son of a stay-home mother and a primary school teacher in Nkhata Bay, started making ‘tough decisions’ very early in life. At a tender age of 13, he and his elder brother Justin left their home on foot, and walked 18 miles with no shoes, to look for what would eventually be their family’s home in search of a better education for him and his siblings.
This was only the beginning of the ‘tough decision making’ that Dr Mkanda is well-known for today. The young Pascal Mkanda continued with his education and was eventually identified as his district’s best performing student. At the time, the president of Malawi, His excellency Dr Hastings Kamuzu Banda, had initiated a programme offering the brightest pupils (top 2.5%) from each district in Malawi irrespective of sex or socio-economic status, the opportunity to attend higher education, at the prestigious Kamuzu Academy, and through this educational opportunity, Dr Mkanda performed exceptionally and was awarded a full sponsorship to study Medicine in the United Kingdom where he attained a medical degree at the Imperial University College London.
To just show how intelligent he was – Pascal was afforded an opportunity to also study for a degree in microbiology/infectious diseases at the London School of Hygiene and Tropical Medicine while at the same time pursuing a degree in medicine. In later life he went to the Rollins School of Public Health at Emory University in Atlanta, USA, and obtained a Master of Public Health.
Putting his theoretical knowledge into practical experience, it was not long before Dr Mkanda began making a very real impact on Malawi’s public health system, improving the health and lives of remote communities. He rapidly developed a reputation for solid, practical and effective work. Here he developed the traits that would characterize his entire career and for which he became so respected: the courage of standing up for his convictions; an ability to identify and promote new and excellent talent, that would help him establish relevant and pragmatic support teams across the region; a fearless dedication to step out of group thinking even if it meant standing alone against adversity; and, an absolute and unwavering commitment to achieving results.
Respected by peers and more importantly communities themselves, he rapidly caught the attention of the international development community while working in some of the most remote communities in Malawi. During a visit by the USAID Mission in Malawi to Nsanje District Hospital in the south of Malawi, Dr Mkanda’s work caught the attention of the Country Representative who immediately recommended him for a USAID-sponsored Global Health Programme which subsequently led to the beginning of his international career.
Starting out as a National Programme Officer in Malawi for the World Health Organization, and moving on to Zambia as an international staff, he met and established a long-term friendship with Dr Francis Kasolo (former VPD Regional Virologist). By the year 2000, Dr Mkanda was managing immunization activities for Eastern and Central Africa and would eventually lead polio activities in Nigeria and Ethiopia.
It was during his time as WHO Polio team leader in Nigeria and Ethiopia that these countries were able to make significant inroads in interrupting wild polio transmission. One contributing factor for this achievement was the introduction of the famous accountability framework that held every staff accountable for their work with those underperforming being replaced by “fresh legs on the football field”, in Pascal’s own words.
It was therefore not a surprise that when the position of WHO African regional polio coordinator was advertised, that Dr Moeti – then the new Regional Director for Africa – appointed Pascal to lead the fight against this disease in the Region.
Never losing focus on the need to reach every last child with polio vaccines, with support from Dr Moeti and the Bill and Melinda Gates Foundation, Dr Mkanda established a regional center for the Geographic and Information Systems (GIS). According to Dr Joseph Cabore, Director of Programme Management at WHO’s African Regional Office: “One very critical contribution by Pascal to the regional office, is the introduction of innovative technologies and solutions. It’s amazing to see in real time, where our frontline workers can reach during mass campaigns and outreach activities. Pascal, thank you for ensuring that we remain accountable to our African children and their families.”
“It has been a privilege to work alongside Dr. Mkanda in pursuit of a polio-free world,” said Dr. Chris Elias, President of Global Development, the Bill & Melinda Gates Foundation. “His commitment and dedication to eradicating polio have been vital to helping protect millions of children from this debilitating disease and helped achieve a WHO African Region that is now free of wild polio – a monumental achievement in global health. I am forever grateful to Dr. Mkanda for his work and partnership on ending polio.”
Michael Galway, Deputy Director Polio at the Bill & Melinda Gates Foundation, added this personal comment: “Working with Pascal over the past decade has been one of best parts of the job in helping to get rid of polio in Africa. I’ve always appreciated the passion and conviction he’s brought to the work, and his keen understanding of how to get the polio programme to perform at its best in some of the most difficult places. He’s been a role-model and a friend, and I’m grateful for both!”
It was in Nigeria – for a long time the global epicentre for polio – that Pascal’s leadership really came into its own.
Dr Faisal Shuaib, Executive Director of the National Primary Healthcare Development Agency in Nigeria, said: “Pascal Mkanda’s contribution to making Nigeria free of wild poliovirus cannot be overstated. It took innovative strategies and approaches to ensure that every child could be reached, and virus transmission effectively tracked, in hard-to-reach and inaccessible areas. Pascal helped develop and trailblaze novel approaches which ultimately led to our success. It really took rewriting the strategic rulebook, and these approaches are now being implemented in other high-risk polio areas. All for the benefit of the most marginalized children. Thank you, Pascal, we could not have done it without you and your leadership. We will miss you!”
Indeed, it is this same leadership by Dr Mkanda that led to the establishment of the Rapid Response Team (RRT), coordinated by Dr Ndoutabe Modjirom in the WHO Regional Office in Brazzaville to tackle the remaining form of polio, the circulating vaccine-derived polioviruses (cVDPVs): “Pascal, you are leaving big shoes to fill. We will need your kind of leadership to end all remaining forms of polio in our region once and for all. It will not be easy to finish this job without you.”
Pascal will be missed, as underscored by Aidan O’Leary, Director for the Global Polio Eradication at WHO Geneva. “On behalf of all partners and stakeholders, the Global Polio Eradication Initiative wishes you all the very best in your retirement and/or in your next chapter of life. We know of course that you will stay engaged in one capacity or another in this fight, and we look forwards to one day, very soon, to celebrate together with you the victory over all forms/types of polio worldwide once and for all. A big thank you, in particular for your leadership in certifying the Region free of wild polioviruses and for facilitating the introduction and roll-out of novel oral polio vaccine type 2.”
Congratulations on your retirement! Now you’ll have more time for sleeping in, fishing, reading, golfing and if you want to be a DJ-from G22, where it all started!
Shine on, le Mystique Dr Mkanda!
26 August 2021, Brazzaville – Governments from the World Health Organization (WHO) African Region have committed to ending all remaining forms of polio and presented a scorecard to track progress towards the eradication of the virus. The commitments came at a dedicated meeting on polio at the Seventy-first WHO Regional Committee for Africa.
While the African Region was certified free of wild poliovirus one year ago following four years without a case, outbreaks of circulating vaccine-derived poliovirus (cVDPV) continue to spread. cVDPVs occur in communities where not enough children have received the polio vaccine. Cases increased last year in part because of disruptions to polio vaccination campaigns caused by COVID-19. Since 2018, 23 countries in the region have experienced outbreaks and more than half of the global 1071 cVDPV cases were recorded in Africa.
“As Chair of the African Union, I am determined to work with other countries to protect the gains of our monumental efforts against polio and finish the job against all forms of this disease in Africa. Only then, we will be able to say we delivered on our promise of a safer, healthier future for all our children,” said H.E. Félix Tshisekedi, President of the Democratic Republic of the Congo.
At the Regional Committee, countries discussed how they will begin implementing the new Global Polio Eradication Initiative (GPEI) 2022-2026 Strategy that was launched in June to urgently stop the spread of cVDPVs. The tools and tactics outlined in the Strategy to stop outbreaks include:
Improving the speed and quality of outbreak response, including through the rapid deployment of surge staff from the WHO Regional Office for Africa to support countries as soon as outbreaks are detected.
Further integrating polio campaigns with the delivery of essential health services and routine immunization to reach children who have never been vaccinated, help build trust with communities and improve uptake of the polio vaccine.
Broadening the rollout of the novel oral polio vaccine type 2 (nOPV2), a new tool that could more sustainably end outbreaks of type 2 cVDPV, which are the most prevalent. To date, six countries in Africa have rolled out the vaccine with close to 40 million children vaccinated and no concerns noted for safety.
“The poliovirus disregards and defies borders. Its presence anywhere in our region is a threat to all countries. Togo is committed to working with our regional partners and acting with the urgency required to implement high quality polio campaigns and protect children across Africa. With collective action, we will defeat all forms of polio,” said Hon Professor Moustafa Mijiyawa, Togo’s Minister of Health and Public Hygiene and Universal Access to Health Care and the Chairperson of the Seventy-first session of the Regional Committee for Africa.
The scorecard presented at the Regional Committee will track indicators for implementation of timely, high-quality polio outbreak response, readiness to introduce nOPV2 as the new vaccine becomes eligible for broader use, strengthening routine immunization to close immunity gaps, and transitioning polio assets into national health systems in a strategic, phased approach. Ministers committed to regularly reviewing progress together on each of these indicators to ensure collective success in urgently finishing the job on polio and securing a polio-free future for every child across the region.
“Our success in ending wild poliovirus in the region shows what is possible when we work together with urgency. COVID-19 has threatened this triumph as governments worked hard to limit the spread of COVID-19, pausing some campaigns. However, we cannot waver, and with renewed vigour we can overcome the final hurdles that jeopardize our success. We have the know-how, but it must be backed by committed resources to reach all under-vaccinated communities and ensure that all children thrive in a world free of polio. Together, we can help the world achieve polio eradication,” said Dr Matshidiso Moeti, WHO Regional Director for Africa.
Almost 100 million African children have been vaccinated against polio since July 2020, after activities were paused due to the COVID-19 pandemic.
The Regional Committee also discussed how to accelerate the transition of polio infrastructure into countries’ health systems, so that it can continue to support immunization and disease surveillance once polio is eradicated. The polio programme has a history of supporting the response to emerging health threats in the Region, including Ebola and COVID-19, and half of polio surge staff are currently helping countries with COVID-19 surveillance, contact tracing and community engagement.
“We need increased political and financial commitment by governments and partners to walk the last mile towards ending all forms of polio,” said Dr Tunji Funsho, chair of Rotary’s National PolioPlus Committee, Nigeria. “We must reach more children faster and comprehensively to not only curb outbreaks swiftly, but to also scale up vaccination coverage and give children lasting protection against this preventable disease.”
Dr Moeti spoke during a virtual press conference today facilitated by APO Group. She was joined by Hon Professor Moustafa Mijiyawa and Dr Tunji Funsho. Also on hand to respond to questions were Dr Pascal Mkanda, Coordinator, Polio Eradication Programme, WHO Regional Office for Africa; Dr Richard Mihigo, Coordinator, Immunization and Vaccines Development Programme, WHO Regional Office for Africa; and Dr Thierno Balde, Team Leader, Operational Partnerships, WHO Regional Office for Africa.
The WHO Regional Committee for Africa is the World Health Organization’s decision-making body on health policy in the African Region. It comprises of Ministers of Health or their representatives from each of the 47 Member States in the African Region.
The Global Polio Eradication Initiative is a public-private partnership led by national governments with six core partners – the World Health Organization (WHO), Rotary International, the US Centers for Disease Control and Prevention (CDC), UNICEF, the Bill & Melinda Gates Foundation and Gavi, the Vaccine Alliance.
For Additional Information or to Request Interviews, Please contact:
13 March 2021, Brazzaville – To rapidly and sustainably stop outbreaks of circulating vaccine-derived poliovirus type 2 (cVDPV2) in African countries, a modified vaccine, known as novel oral polio vaccine type 2 (nOPV2) is now being rolled out.
Last year, on 25 August 2020, Africa made history with the African Region Certification Commission for Polio Eradication independently certifying that the Region was free of wild poliovirus. This is the second disease to be kicked out of Africa after smallpox more than 40 years ago.
This achievement is remarkable, considering that in the 1990s wild poliovirus paralysed more than 75,000 African children every single year – a situation that prompted Nelson Mandela in 1996, joined by Rotary International and other partners, to issue a stark call to action: Kick Polio Out of Africa!
All strains of wild poliovirus have now been interrupted in the continent. The last case of wild poliovirus was in August 2016.
However, this tremendous progress remains an unfinished success story. Although Africa is free of wild poliovirus, countries continue to be affected by another form of the virus, known as circulating vaccine-derived poliovirus type 2 (cVDPV2). Such strains are rare, but can occur in under-immunized communities with limited access to safe water and sanitation.
Populations that are adequately immunized are protected from both wild and vaccine-derived strains of poliovirus. However, because of gaps in immunization coverage across Africa, 20 countries have been affected by cVDPV2 outbreaks since 2018.
Now, intensified efforts are being launched to finish polio once and for all, to ensure no child in Africa will ever be paralysed by any strain of this virus.
The novel OPV2 vaccine has been in development since 2011, and in November 2020, WHO’s Prequalification Team issued an emergency use listing (EUL) recommendation enabling initial roll-out in countries affected by cVDPV2 outbreaks. Soon after the issuance of the EUL, the WHO Regional Director for Africa, Dr Matshidiso Moeti, advocated to countries to use this additional tool to stop all forms of polio in Africa.
For nOPV2 to be deployed and used under the EUL, special readiness requirements and criteria need to be met. The Polio Rapid Response Team at WHO’s Regional Office for Africa, in close coordination with other Global Polio Eradication Initiative partners, has been working intensely with countries and partners across the continent to respond to outbreaks of cVDPV2 and prepare for the roll out of nOPV2.
As countries in the Region gear up to roll out this new tool for outbreak response, with WHO’s support they are developing supply, demand and deployment plans; ensuring expedited pathways for national regulatory approvals; enhancing surveillance and laboratory capacity; investing in meeting cold-chain capacity and vaccine management requirements; ensuring vaccine safety monitoring and follow-up mechanisms are in place; and developing communication plans and engaging communities to enhance understanding of the vaccine and risks posed by cVDPV2.
These preparations continue even amidst the COVID-19 pandemic, and the existing polio eradication infrastructure has been instrumental in preparing for the nOPV2 vaccine as well as more broadly supporting COVID-19 response efforts across the continent.
Years of extensive development and preparations are now about to pay off, as nOPV2 will now be utilized for outbreak response. “This is tremendous news for Africa’s polio eradication effort, and in particular for Africa’s children who are currently at risk of lifelong paralysis due to circulating vaccine-derived poliovirus,” said Dr Moeti. “This tool can stop cVDPV2 but only if it reaches all at-risk children. We must apply the lessons from the decades of action to kick wild polio out of Africa. This will require the collective action of political leaders, traditional and religious leaders, public health experts, partners, donors, frontline health workers and of course parents and caregivers. Together, we can protect all African children from all forms of this virus.”
N’Djamena – One of the largest polio immunization campaigns in the African Region this year has just concluded in Chad, where over 3.3 million children in 91 districts were vaccinated. This pushes the total number of children vaccinated against polio to over forty million across 16 countries in the Region, since campaigns resumed following a necessary pause in immunizations due to the COVID-19 pandemic.
While Africa was declared free of the wild poliovirus in August 2020, another form of polio continues to affect children: circulating vaccine-derived poliovirus, or cVDPV. This type of polio is rare and can only occur in areas where not enough children are immunized. The only way to stop spread of cVDPV is through immunization.
The current type 2 cVDPV outbreak in Chad was detected in February 2020—yet immunizations were halted due to COVID-19 and the virus spread to 36 districts across the country, paralyzing more than 80 children and even leading to cases in neighbouring Sudan and the Central African Republic.
“Viruses do not respect national borders,” said Dr Ndoutabé Modjirom, head of the polio Rapid Response Team at the World Health Organization (WHO) African Region. “Given Chad’s central geographic location and its mobile populations, it was important to carry out a large-scale campaign that targeted key populations and high-risk areas throughout the country.”
The vaccination campaign was carried out in two phases, the first taking place between 13-15 November and the second from 27-29 November.
While mass polio vaccination campaigns were stopped across Africa due to COVID-19 restrictions, they resumed in July 2020. The response in the region overall, and in Chad in particular, demonstrates the commitment by Global Polio Eradication Initiative partners and countries across Africa to stop polio, even amidst the difficult operating context of COVID-19.
“The number of children reached since polio campaigns have resumed is extremely encouraging,” said Dr Matshidiso Moeti, WHO Regional Director for Africa. “This large-scale campaign in Chad during COVID-19 is a reflection of the Region’s commitment and ability to face multiple difficult health challenges and protect the health of all children.”
Although campaigns were on hold for several months, work did not stop. Chad’s team of national and international polio experts together with the AFRO Rapid Response Team tracked the virus, conducted a comprehensive risk assessment, and planned an outbreak response to take place as soon as it was safe to do so, taking into account timelines in outbreak response standards of practice. Consultations were also held with the national COVID-19 task force to ensure that best practices in infection prevention and control would be followed. The commitment and efforts of the Ministry of Health and other key national and regional health leaders and partners, including UNICEF, were instrumental in conducting the campaign.
“With increased immunizations and the continued commitment of health leaders and partners, we are confident that we will soon see the end of this outbreak and the end of all forms of polio in Africa,” said Dr Jean Bosco Ndihokubwayo, WHO representative for Chad.
About polio eradication
The Global Polio Eradication Initiative is spearheaded by WHO, Rotary International, the US Centers for Disease Control and Prevention (CDC), UNICEF, the Bill & Melinda Gates Foundation and Gavi, the Vaccine Alliance.
On 6 November, WHO and UNICEF jointly issued an urgent call to action to avert major measles and polio epidemics as COVID-19 continues to disrupt immunization services worldwide, leaving millions of vulnerable children at heightened risk of preventable childhood diseases. Learn more about the call to action.
In a year marked by the global COVID-19 pandemic, global health leaders convening virtually at this week’s World Health Assembly called for continued urgent action on polio eradication. The Assembly congratulated the African region on reaching the public health milestone of certification as wild polio free, but highlighted the importance of global solidarity to achieve the goal of global eradication and certification.
Member States, including from polio-affected and high-risk countries, underscored the damage COVID-19 has caused to immunization systems around the world, leaving children at much more risk of preventable diseases such as polio. Delegates urged all stakeholders to follow WHO and UNICEF’s joint call for emergency action launched on 6 November to prioritise polio in national budgets as they rebuild their immunization systems in the wake of COVID-19, and the need to urgently mobilise an additional US$ 400 million for polio for emergency outbreak response over the next 14 months. In particular, Turkey and Vietnam have already responded to the call, mobilising additional resources and commitments to the effort.
The Assembly expressed appreciation at the GPEI’s ongoing and strategic efforts to maintain the programme amidst the ‘new reality’, in particular the support the polio infrastructure provides to COVID-19-response efforts. Many interventions underscored the critical role that polio staff and assets play in public health globally and underline the urgency of integrating these assets into the wider public health infrastructure.
At the same time, the GPEI’s work on gender was recognized, with thanks to the Foreign Ministers of Australia, Spain and the UK for their roles as Gender Champions for polio eradication.
Delegates expressed concern at the increase in circulating vaccine-derived poliovirus (cVDPV) outbreaks, and urged rapid roll-out of novel oral polio vaccine type 2 (nOPV2), a next-generation oral polio vaccine aimed at more effectively and sustainably addressing these outbreaks. This vaccine is anticipated to be initially rolled-out by January 2021.
Speaking on behalf of children worldwide, Rotary International – the civil society arm of the GPEI partnership – thanked the global health leaders for their continued dedication to polio eradication and public health, and appealed for intensified global action to address immunization coverage gaps, by prioritizing investment in robust immunization systems to prevent deadly and debilitating diseases such as polio and measles.
Dr. Tunji Funsho, chair of Rotary’s Nigeria National PolioPlus Committee, joins 100 pioneers, artists, leaders, icons, and titans as one of TIME’s 100 Most Influential People. TIME announced its 2020 honorees during a 22 September television broadcast on ABC, recognizing Funsho for his instrumental leadership and work with Rotary members and partners to achieve the eradication of wild polio in the African region.
He is the first Rotary member to receive this honor for work toward eradicating polio.
A Rotarian for 35 years, Funsho is a member of the Rotary Club of Lekki, Nigeria, past governor of District 9110, and serves on Rotary’s International PolioPlus Committee. Funsho is a cardiologist and a fellow of the Royal College of Physicians of London. He lives in Lagos, Nigeria with his wife Aisha. They have four children; Habeeb, Kike, Abdullahi and Fatima; and five grandchildren.
TIME 100 comprises individuals whose leadership, talent, discoveries, and philanthropy have made a difference in the world. Past honorees include Bono, the Dalai Lama, Bill Gates, Nelson Mandela, Angela Merkel, Oprah Winfrey, and Malala Yousafzai.
After the World Health Assembly passed a resolution to eradicate polio worldwide in 1988, the Global Certification Commission led the way in establishing a formal certification process, asking each of the six WHO regions to set up a Regional Certification Commission. Then in 1996, the WHO Regional Director for Africa created the Africa Regional Certification Commission (ARCC) for Polio Eradication: a 16-person independent body tasked with overseeing this process, and later on containment activities in the African region.
Professor Rose Leke, an infectious disease specialist, has been the chairperson of the ARCC since it was set up in 1998. A trailblazer for women in global health, Leke has fought throughout her career to improve women’s representation in science and global health leadership. In 2018, she was one of nine women honored with a Heroine of Health award, recognizing her outstanding contribution to health care.
Stopping the ‘havoc’ of polio in Africa
Professors Leke explains her motivation to join the polio eradication cause, “When I was invited to be part of the ARCC in 1998, I was not involved in any polio-related work. But I could see the havoc that polio was reaping on the continent. I had a nephew who was paralyzed from polio and suffered brain damage, and another relative who contracted polio and continues to inspire me. Back then, you saw so many paralyzed young people on the streets. You don’t see that today.”
Ridding the African continent of wild poliovirus is a huge achievement, many years in the making. Nigeria, the last bastion of the wild virus, proved a particularly tough setting in which to vaccinate every child and ensure that no trace of the virus remained.
Professor Leke reflects, “It’s been such a long road. When Nigeria didn’t report any cases of wild polio for two years between 2014 to 2016, we were apprehensive but satisfied. We were so close to eradication as a region, everything was going so well, and then wild polio was reported again in Nigeria in August 2016, and certification had to go on the back burner.”
“The Nigerian response to their outbreaks has been extraordinary. Everyone is committed and highly involved. In Sokoto and Kano states, where I was recently for a field verification visit, and in all other states, everyone – from government officials, traditional leaders, health staff and field teams, community health workers and informants, polio survivors to traditional birth attendants – was heavily engaged in the response. The innovative technologies that have emerged have similarly been incredible. The Nigerian Emergency Operations Centre is a well-coordinated structure that is behind Nigeria’s success. Other disease programs in Africa are learning from this.”
Professor Leke never lost her drive to end polio, even during difficult years and despite the tough choices her role sometimes presented.
“When we started, we were aiming for wild polio to be eradicated by 2000; the thought of this success really kept me motivated and still does. At times it has been a huge sacrifice; as Temporary Advisers, ARCC members are not paid, and I’ve sometimes given up consultancies to do this work. My husband, children and grandchildren will tell you, there was a huge amount of traveling and many meetings. But I don’t regret the time spent for a moment on such a cause.”
“When Dr Moeti was appointed as WHO Africa Regional Director in 2011, this was further motivation to continue: I wanted to support a fellow woman. In the beginning, I was the only female in the Global Certification Commission. The commission has addressed this imbalance and we are now two females out of the six members. We need more women in senior positions on the African continent.”
Fighting for gender equality in global health and science
In 2011, Professor Leke won the Kwame Nkrumah Award for the best female scientist in Central Africa for her research on malaria. As part of her acceptance of the award, she took a pledge “to help promote the participation of women in science in Cameroon.”
Within a year, she had helped set up HIGHER Women, a mentoring programme for senior female scientists to deliver hard and soft skills training to their early career counterparts. To support the programme, Professor Leke contributed some of her own funds.
Professor Leke says, “As a woman I encountered blocks on the way during my career – at times men asked me to leave the laboratory space I was working in.”
“Science can be a pyramid – there are many early women researchers, but far fewer at the top of the field. Research and academia have a ‘publish or perish’ culture which disadvantages women who have responsibilities outside of the lab – such as raising a family.”
Professor Leke has continually used her position to promote women in science and global health, even sharing her favorite motivational track about women’s empowerment.
Whilst great progress towards gender balance has been made since she started her career, Professor Leke is firm in noting that there is more to do. In the African regional polio programme, women still lead only a small number of national committees.
Professor Leke is proud of the public health legacy that the polio eradication programme will leave in the African region. She says, “The polio response has brought many skilled technicians into Africa’s health systems. The GPEI paved the way for working closely with traditional healers and community leaders and has really helped to strengthen the systems that report on other diseases. The polio laboratory network is being used for other diseases, giving capacity in the region for doing all sorts of other diagnostics. You’ll find the one person in the health center who was there for polio is reporting on many other diseases.”
“After we declare Africa as free of the wild poliovirus, the ARCC will work with countries to ensure they keep up good quality surveillance, and improve routine immunization, keeping population immunity as high as possible. We will also continue to guide countries in continuing to monitor population immunity to prevent importations of wild poliovirus from outside the African region, while ensuring that the threat of circulating vaccine derived polio viruses (cVDPVs) is addressed.”
“Our work continues until all forms of polio have been eradicated globally.”
GENEVA, 25 August 2020 – Today, the Africa Regional Certification Commission certified the WHO African Region as wild polio-free after four years without a case. With this historic milestone, five of the six WHO regions – representing over 90% of the world’s population – are now free of the wild poliovirus, moving the world closer to achieving global polio eradication.
Only two countries worldwide continue to see wild poliovirus transmission: Pakistan and Afghanistan.
The Global Polio Eradication Initiative (GPEI) congratulates the national governments of the 47 countries in the WHO African Region for today’s achievement.
“Ending wild polio virus in Africa is one of the greatest public health achievements of our time and provides powerful inspiration for all of us to finish the job of eradicating polio globally,” said WHO Director-General Dr Tedros Adhanom Ghebreyesus. “I thank and congratulate the governments, health workers, community volunteers, traditional and religious leaders and parents across the region who have worked together to kick wild polio out of Africa.”
Strong leadership and innovation were instrumental in stopping the wild poliovirus in the region. Countries successfully coordinated their efforts to overcome major challenges to immunizing children, such as high levels of population movement, conflict and insecurity restricting access to health services, and the virus’s ability to spread quickly and travel across borders.
In addition, the continued generosity and shared commitment of donors – including governments, the private sector, multilateral institutions and philanthropic organizations – to achieving a polio-free world helped build the infrastructure that enabled the African region to reach more children than ever before with polio vaccines and defeat wild polio.
“During a challenging year for global health, the certification of the African region as wild poliovirus-free is a sign of hope and progress that shows what can be accomplished through collaboration and perseverance,” said Rotary International President Holger Knaack. “Since 1996, when Nelson Mandela joined with Rotary, the Global Polio Eradication Initiative, and governments of the African region we’ve achieved something remarkable. Today’s milestone tells us that polio eradication is possible, as long as the world remains committed to finishing the job. Let us work together to harness our collective energies to overcome the remaining challenges and fulfil our promise of a polio-free world.”
The resources and expertise used to eliminate wild polio have significantly contributed to Africa’s public health and outbreak response systems. The polio programme provides far-reaching health benefits to local communities, from supporting the African region’s response to COVID-19 to bolstering routine immunization against other vaccine-preventable diseases.
While this is a remarkable milestone, we must not become complacent. Continued commitment to strengthening immunization and health systems in the African region is essential to protect progress against wild polio and to tackle the spread of type 2 circulating vaccine-derived poliovirus (cVDPV2), which is present in 16 countries in the region. Pockets of low immunity mean such strains continue to pose a threat and the risk is magnified by interruptions in vaccination due to COVID-19, which have left communities more vulnerable to cVDPV2 outbreaks.
The GPEI calls on countries and donors to remain vigilant against all forms of polio. Until every strain is eradicated worldwide, the incredible progress made against polio globally will be at risk.
The WHO African Region’s success against wild polio has shown the world that progress against some of the biggest global health challenges is possible. The GPEI is grateful for every person, partner, donor and country who helped bring about this incredible achievement.
Media contacts:
Oliver Rosenbauer
Communications Officer, World Health Organization
Email: rosenbauero@who.int
Tel: +41 79 500 6536
The Global Polio Eradication Initiative is a public-private partnership led by national governments with six core partners – the World Health Organization (WHO), Rotary International, the US Centers for Disease Control and Prevention (CDC), UNICEF, the Bill & Melinda Gates Foundation and Gavi, the Vaccine Alliance.
For information and multimedia content on the WHO African Region’s efforts to eradicate wild polio, please visit africakicksoutwildpolio.com.
The WHO African Region is expected to be certified free of wild poliovirus on 25 August 2020. Chair of the WHO’s International Health Regulations Emergency Committee and of the AFRO Regional Immunization Technical Advisory Group Helen Rees explains the current cVDPV situation in Africa and its implications ahead of regional wild polio-free certification.
Q. Fifteen countries (as of 14 August 2020) in the World Health Organization’s African region have reported cases of circulating vaccine-derived polio type 2 (cVDPV2) in 2020. The total number of outbreak countries is 16. How does that impact the region’s upcoming wild polio-free certification?
First, it’s important to clarify that cVDPV is a different virus from the wild poliovirus, and will undergo a separate process to validate its absence once wild polio has been eradicated globally.
Second, I want to underscore that the ongoing cVDPV2 outbreaks in Africa do not affect the programme’s confidence that wild polio is gone from the region. Certification is backed by extensive data and a thorough evaluation process that demonstrates wild polio transmission has been interrupted on the continent.
In Africa, an independent body of experts called the African Regional Certification Commission for polio eradication (ARCC) oversees this process by carefully reviewing country documentation and analyzing the quality of surveillance systems and immunization coverage. With this intensive monitoring of polio programmes across the continent, the ARCC is able to confirm with 100% certainty that wild polio is gone from the region.
But for the ARCC, national polio programmes and GPEI partners, the work does not end here. Stopping cVDPVs remains an urgent priority. African countries will need to strengthen their efforts to reach all children with polio vaccines to protect them from cVDPVs and any importation of wild polio from the remaining endemic countries, Pakistan and Afghanistan.
How do cVDPV outbreaks happen?Andwhy has the number of cVDPV cases in Africa increased more rapidly in the past couple years while wild cases have not?
cVDPVs can occur if not enough children receive the polio vaccine. In under-immunized populations, the live weakened virus in the oral polio vaccine (OPV) can pass between individuals and, over time, change to a form that can cause paralysis—resulting in cVDPV cases. This means that the cVDPV outbreaks we’re seeing today are revealing pockets across the continent where immunization rates are too low.
The reason for the increase in cases can be explained by low immunity to type 2 poliovirus, which causes the vast majority of cVDPV cases. This is in part due to a global vaccine switch that occurred in 2016, when countries stopped using the trivalent OPV (which protects against all three forms of polio) and replaced it with the bivalent OPV (which protects against just type 1 and 3).
The GPEI, following the advice of the Strategic Advisory Group of Experts, decided to make this vaccine switch based on extensive evidence that showed it would decrease the number of cVDPV outbreaks. However, immunity to type 2 poliovirus was lower than predicated at the time of the switch and so there were actually more cVDPV2 outbreaks. In response to the cVDPV2 outbreaks monovalent oral polio vaccine type 2 (mOPV2) has been used to interrupt transmission. But with increasing numbers of children who do not have type 2 immunity, mOPV2 vaccines have had to be used longer and in larger quantities than was initially anticipated. This larger and more extensive use of mOPV2 vaccines has seeded new outbreaks especially in areas of low immunization coverage and on the borders of outbreak response zones.
All this said, mOPV2 is an effective tool to stop cVDPV outbreaks if children are properly immunized.
If cVDPV outbreaks can only affect under-immunized communities, doesn’t the increasing number of outbreaks indicate that polio immunity levels are too low across the region? Why were countries able to stop wild polio then?
For years, the wild poliovirus has only existed in a small area on the continent. Nigeria reported its last case of paralysis due to wild polio four years ago, but most other countries haven’t seen a wild polio case in quite some time.
Across the continent, population immunity levels to type 1 polio (the only type of wild polio that remains in the world) and surveillance networks have continued to protect against any wild polio importation from remaining wild polio endemic countries.
However, the increasing number of cVDPV outbreaks across Africa is a reminder that countries cannot afford to let their guard down, and must continue reaching every child with the polio vaccine.
What is the programme doing to address cVDPVs in Africa?
The same tactics that stop wild polio can be used to stop cVDPVs – high vaccination coverage and strong surveillance. The polio programme in Africa has proven experience and strategies to address cVDPV outbreaks. But we know that we cannot rely only on existing tactics, which is why the programme is innovating and adapting its strategies to address the challenge of cVDPVs specifically.
In early 2020, the GPEI released a comprehensive new strategy to stop cVDPV outbreaks currently affecting countries in Africa, Asia and the Middle East.
This includes revising outbreak response standard operating procedures to improve response time, doubling the size of the African Rapid Response Team, forming a global Rapid Response Team and prioritizing the GPEI’s ground presence in high-risk areas.
To raise immunization coverage, the GPEI partners – including Gavi, the Vaccine Alliance – are working to build and strengthen immunization systems in at-risk countries and expand routine immunization with the inactivated polio vaccine (IPV).
The strategy also includes the development of an additional tool to help stop cVDPV2 outbreaks – novel oral polio vaccine type 2 (nOPV2). nOPV2 is a modified version of the existing mOPV2 used to respond to cVDPV2 outbreaks that is less likely to change to a form that can cause paralysis.
The GPEI is confident that with strengthened commitment from country governments and full implementation of the tactics laid out in its strategy, cVDPVs can be wiped out across Africa.
Has COVID-19 affected the programme’s ability to stop cVDPV outbreaks in the region?
The recent pause in house-to-house polio campaigns to help control the spread of COVID-19 is expected to increase cVDPV transmission across affected countries.
The GPEI is taking a number of steps to get back on track. Even while campaigns were paused, surveillance activities continued so that as immunization activities ramp up the programme can target campaigns in areas that are most at risk.
The GPEI recently recommended that all countries with active polio transmission resume vaccination activities as soon as it is safe to do so, in line with WHO and national COVID-19 guidance. Burkina Faso and Angola were among the first countries to start implementing cVDPV outbreak response campaigns after the pause.
These campaigns are closely following safety guidelines and social distancing measures to protect communities and health workers against COVID-19. Measures including the use of masks and gloves, frequent handwashing and no-touch vaccination.
COVID-19 undoubtedly represents a setback for polio eradication, but not the first one the programme has faced. The GPEI and African countries’ national polio programmes are committed to ensuring that countries are ready to tackle the remaining challenge of cVDPVs and to recover lost ground once polio activities can safely ramp up.
Click on the image for information and multimedia content.
Expertise in polio eradication that has put Africa on the verge of being certified free of wild poliovirus has been brought to the frontlines of the COVID-19 fight. A network of responders from the World Health Organization (WHO) polio eradication programme and partner organizations is providing critical resources and skills to tackle the COVID-19 pandemic.
To boost testing in the WHO African Region, the WHO-coordinated polio laboratory network comprising 16 laboratories in 15 countries is now dedicating 50% of its capacity to COVID-19 testing. Hundreds of tests are carried out every day using polio testing machines in Algeria, Cameroon, Cote d’Ivoire, Ethiopia, Madagascar, Nigeria, Senegal and South Africa.
“In Africa, no one has the footprint of the polio programme nor the expertise for mounting effective response campaigns. So with COVID-19 threatening to overwhelm health systems, the extensive polio response network is once again lending crucial support as countries build up systems to contain COVID-19,” said Dr Matshidiso Moeti, the WHO Regional Director for Africa.
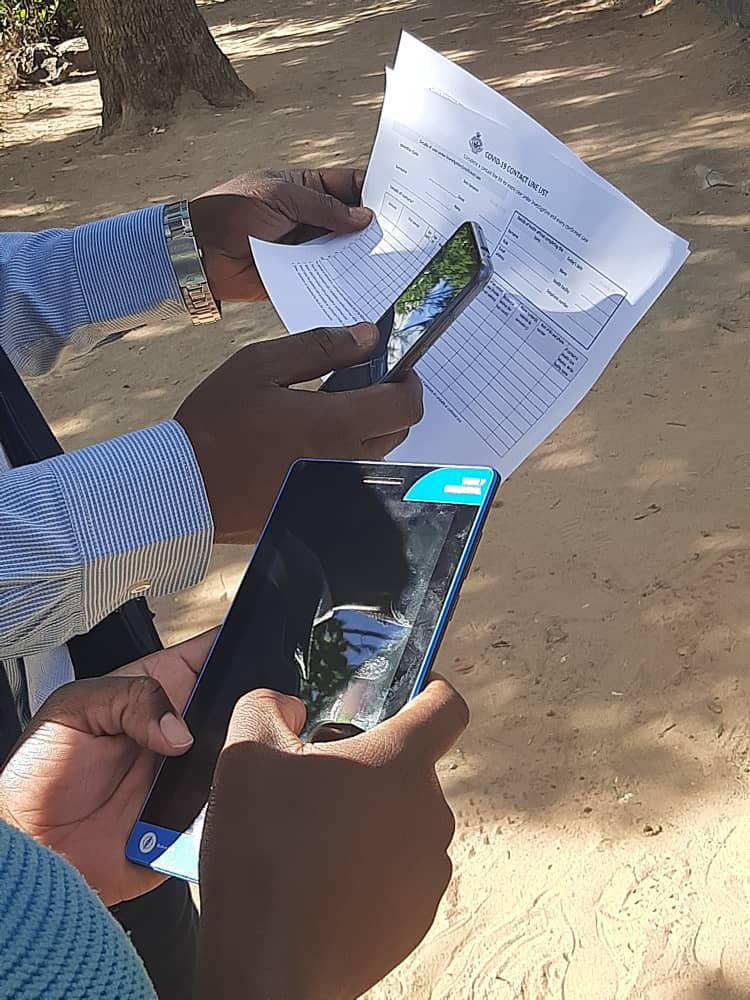
Contact tracing has also been a central pillar of the WHO polio programme’s support to the COVID-19 response. Mobile phone applications originally developed for health workers to use in polio outbreak response and disease surveillance have been adapted by WHO to be used against COVID-19. In Zimbabwe, for example, over 100 disease surveillance officers are using these tools for case investigations and contact tracing in many provinces where COVID-19 has been confirmed.
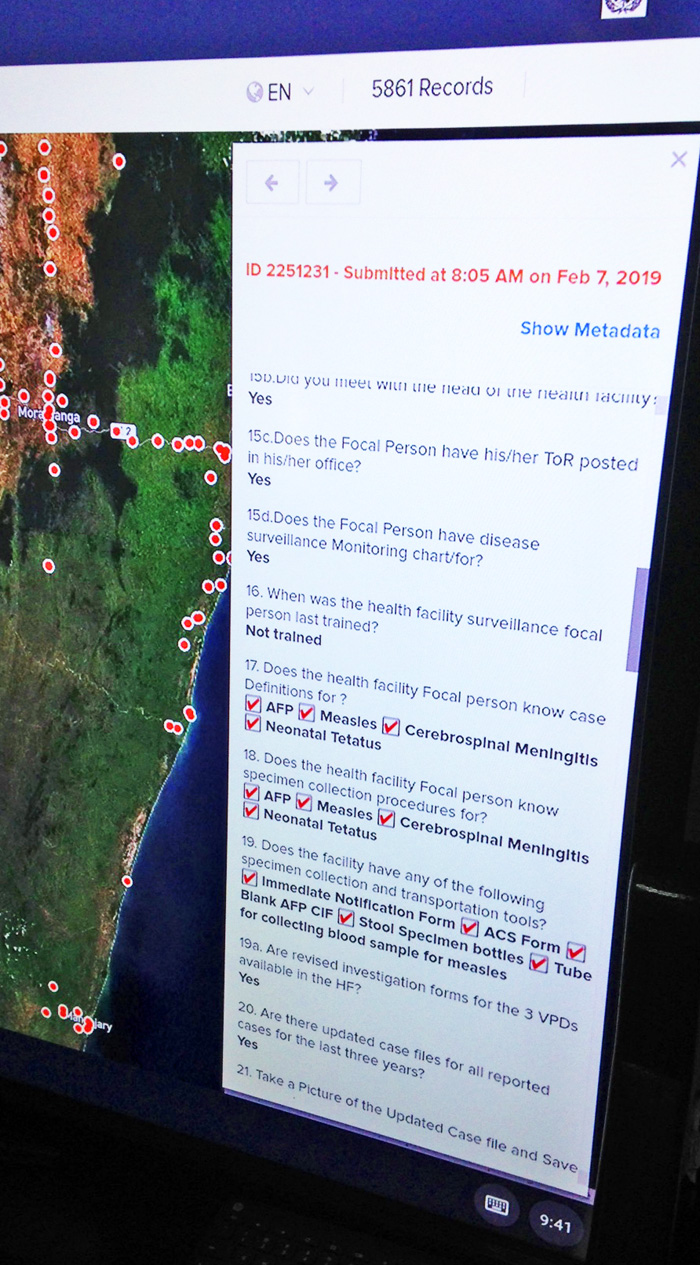
In addition, the WHO Geographic Information System (GIS) centre in Brazzaville, Congo – which was opened in 2017 to support the polio programme with adapted technologies and data management – is using its huge experience in outbreak response and disease surveillance to support countries with a range of GIS and software technology and manual solutions to respond to COVID-19. The GIS team is now working around the clock supporting countries to take up the technology for COVID-19 responses.
More than 2000 polio response experts from WHO, UNICEF, Rotary, as well as STOP consultants from the United States Centers for Disease Control and Prevention are supporting the COVID-19 response in the African Region. A quarter of WHO polio staff are dedicating more than 80% of their time towards COVID-19 efforts, with 65% anticipating a commitment of six months or more.
Alongside the support to the COVID-19 response, WHO polio staff are also maintaining critical functions including disease surveillance and planning to resume mass polio immunization campaigns once the situation permits to reduce the risk of new polio outbreaks.
“It is important that the support to COVID-19 response does not jeopardize the progress made in stopping all forms of polio transmission in the region. The fight against the pandemic should not come at the detriment of other health emergencies,” emphasized Dr Moeti.
Focus: Using digital tools for contract tracing in Zimbabwe
“With Zimbabwe’s first COVID-19 case, we used paper tools to facilitate data management during case investigation and contact tracing, but our contact tracers faced many challenges with follow up and reporting,” says Manes Munyanyi, Deputy Director Health Information and Surveillance Systems for Zimbabwe’s Ministry of Health and Child Care.
“Using digital tools [provided by the polio programme] for outbreak responses cannot be overemphasized as the technology provides responders with data management, visualization and information dissemination platforms that support informed decision making at all levels.”
Using the vast infrastructure developed to identify the poliovirus and deliver vaccination campaigns, the polio eradication programme is pitching in to protect the vulnerable from COVID-19, especially in polio-endemic countries. From Pakistan to Nigeria, the programme is drawing on years of experience fighting outbreaks to support governments as they respond to the new virus.
Pakistan
Few health programmes have as much practice tracking virus or reaching out to communities as the Pakistan polio eradication programme. This means the polio team is in a strong position to support the Government of Pakistan in COVID-19 preparedness and response.
Currently, the polio team is providing assistance across the entire country, with a special focus on strengthening surveillance and awareness raising. Working side-by-side with the Government of Pakistan, within three weeks the team has managed to train over 280 surveillance officers in COVID-19 surveillance. It has also supported the development of a new data system that’s fully integrated with existing data management system for polio. All polio surveillance staff are now doubling up and supporting disease surveillance for COVID-19. Through cascade trainings, they have sensitized over 6,260 health professionals on COVID-19, alongside their polio duties, in light of the national emergency. These efforts will continue unabated as the virus continues to spread.
Adding to the capacity of the government and WHO Emergency team, the polio team are also engaged in COVID-19 contact tracing and improving testing in six reference laboratories. They have been trained to support and supplement the current efforts, preparing for a sudden surge in cases and responding to the increase in travelers that need to be traced as a result of the rise in cases. The regional reference laboratory for polio in Islamabad is also providing technical support to COVID-19 testing and has been evolving to cater to the increased demands.
As this is a new disease, polio staff are lending their skills as health risk communicators – providing accurate information and listening to people’s concerns. The government of Pakistan extended a national help line originally used for polio-related calls to now cater to the public’s need for information on COVID-19. The help line was quickly adapted by the polio communication team once the first COVID-19 case was announced. The polio communications team is using strategies routinely used to promote polio vaccines to disseminate information about the COVID-19 virus, including working with Facebook, to ensure accurate information sharing, and airing television adverts. As time goes on, the teams will train more and more people ensuring the provision of positive health practices messages that can curb the transmission of the virus.
Afghanistan
Currently, community volunteers who work for the polio programme to report children with acute flaccid paralysis (AFP) are delivering messages on handwashing to reduce spread of COVID-19, in addition to polio. UNICEF is similarly using its Immunization Communication Network to disseminate information on personal hygiene.
Field staff have taken the initiative of using their routine visits to health facilities, during which they check for children with AFP, to check for and report people who may have COVID-19. Meanwhile, programme staff are building the capacity of health workers to respond to the novel coronavirus.
To coordinate approaches, the WHO Afghanistan polio team has a designated focal point connecting with the wider COVID-19 operation led by the Government of Afghanistan. The polio eradication teams at regional and provincial levels are working closely with the Ministry of Public Health, non-governmental organizations delivering Afghanistan’s Basic Package of Health Services and other partners to enhance Afghanistan’s preparedness.
Nigeria
“In the field, when there is an emergency, WHO’s first call for support to the state governments is the polio personnel,” says Fiona Braka, WHO polio team lead in Nigeria.
In Ogun and Lagos states, where two cases of COVID-19 have been detected, over 50 WHO polio programme medical staff are working flat out to mitigate further spread, using lessons learnt from their years battling the poliovirus. Staff are engaged in integrated disease surveillance, contact tracing, and data collection and analysis. Public health experts working for the Stop Transmission of Polio programme, supported by the US Centers for Disease Control and Prevention, are using their skills to undertake COVID-19 case investigations.
The WHO Field Offices -which are usually used for polio eradication coordination- are doubling up as coordination hubs for WHO teams supporting the COVID-19 response. The programme is also lending phones, vehicles and administrative support to the COVID-19 effort.
In states where no cases of COVID-19 have been reported, polio staff are supporting preparedness activities. At a local level, polio programme infrastructure is being used to strengthen disease surveillance. Polio staff are working closely with government counterparts and facilitating capacity building on COVID-19 response protocols and are working to build awareness of the virus in the community. Specials efforts are being undertaken to train frontline workers as they are at high risk of contagion.
Beyond polio-endemic countries
Trained specialists in the STOP program, part of the Global Polio Eradication Initiative, are actively supporting preparations or response to COVID-19 in 13 countries worldwide. The WHO Regional Office for Africa’s Rapid Response Team, who usually respond to polio outbreaks, are aiding COVID-19 preparedness in countries including Angola, Cameroon and the Central African Republic. Meanwhile, polio staff in other offices are ready to lend support, or are already lending support, to colleagues working to mitigate and respond to the new virus.
In our work to end polio, the programme sees the devastating impact that communicable diseases have. With this in mind, we are fully committed to supporting national health systems by engaging our expertise and assets to help mitigate and contain the COVID-19 pandemic, alongside continuing concerted efforts to eradicate polio.
For the latest information and advice on the COVID-19 disease outbreak visit the WHO website.
From a small prefabricated container where the walls host detailed maps and desks prop up computer screens beaming data, tables and graphics, the Rapid Response Team at the World Health Organization’s (WHO) Regional Office for Africa coordinate polio outbreak response. The team work across the continent, where 12 countries are battling the vaccine-derived strain of the virus.
Dr Ndoutabe Modjirom, a former Chadian university professor-turned WHO medical officer, coordinates the multi-agency team, which was formed in September 2019. It is composed of twenty experts in operations and vaccination management, epidemiology, logistics, and communications. They are drawn from the core partners of the Global Polio Eradication Initiative (GPEI): WHO, the United Nations Children’s Fund (UNICEF), Rotary International, the US Centers for Disease Control and Prevention, the Bill & Melinda Gates Foundation, and Gavi, The Vaccine Alliance.
The team is mobilized whenever a new polio outbreak is confirmed in the African region.
The first 72 hours
“Our work starts once the lab confirms that a sample collected from either the environment or a paralysed child is caused by a poliovirus. Every minute that passes after the lab confirmation means that the poliovirus is circulating and risks infecting more children,” says Dr Modjirom.
Within the first 72 hours, the Rapid Response Team deploys Team A. This team includes the GPEI Coordinator alongside an epidemiologist, an operations officer, a vaccine manager and a communicator for development. The team works closely with the health authorities in the affected country along with the relevant WHO and UNICEF country offices to prepare a risk assessment and outbreak response plan. The emergency response vaccination campaign, called ‘Round Zero’, starts within 14 days.
Team B takes over from Team A after the first eight weeks and continues the outbreak response activities.
According to standard operating procedures for responding to outbreaks, the polio programme must implement three rounds of high-quality vaccination campaigns in response to every outbreak. Parallel to vaccination, countries must intensify disease surveillance activities to detect new cases of acute flaccid paralysis, a clinical symptom of poliomyelitis.
“Priorities are constantly shifting for the Rapid Response Team,” says Dr Christopher Kamugisha, who has been working with WHO since 1998. He has been a member of the Rapid Response Team since its inception and like the rest of the team has been chasing new polio outbreaks across the region.
“In August I was in Somali Region in Ethiopia supporting the outbreak response, conducting the first vaccination campaign round. On the second day of the campaign, Dr Ndoutabe informed me that a new case was detected in Cheporoni in Ghana and asked me to go and provide technical support,” Dr Kamugisha recalls.
Within 24 hours, he was on a plane to Accra through Addis.
“I arrived at noon the next day and went straight to support the national technical team in their preparations and risk assessment. I assisted with ensuring that their plans are in line with the international standard operating procedures set by the GPEI,” Dr Kamugisha says.
No cure for polio
Polio is a viral disease, multiplying in the intestines and transmitted from person to person mainly through a faecal-oral route or, less frequently, through contaminated water or food.
While there is no cure for polio, the disease can be prevented through administration of a simple and effective vaccine. That is why efforts are underway across the country to rapidly boost immunity levels in children and protect them from polio paralysis.
Thanks to the efforts of the GPEI and country governments, no wild poliovirus has been detected anywhere in Africa since 2016. This stands in stark contrast to 1996, a year when wild poliovirus paralysed more than 75,000 children across every country on the continent.
In 2020, the central challenge for the African Region is overcoming outbreaks of circulating vaccine derived poliovirus. Vaccine-derived polioviruses are rare, but can affect unimmunized and under-immunized populations living in areas with inadequate sanitation and low levels of polio immunization.
Countries experiencing outbreaks of vaccine-derived poliovirus in Africa are Angola, Benin, Cameroon, Central African Republic, Chad, Côte d’Ivoire, Democratic Republic of the Congo, Ethiopia, Ghana, Nigeria, Togo and Zambia. Reasons these outbreaks have occurred include weak routine vaccination systems, vaccine hesitancy, difficulty accessing some locations and low-quality vaccination campaigns, which have made immunization of all children challenging.
In addition to the response activities, the Rapid Response Team work to build the capacity of health workers and decision makers in countries that are not experiencing polio outbreaks, training them to be ready to respond if virus is ever detected.
The team also aims to recruit more women with expertise in outbreak response. Achieving gender balance amongst personnel through a more equitable recruitment process forms part of the GPEI Gender Equality Strategy 2019 – 2023, which was launched in May 2019.
By supporting countries during outbreaks, and building health system resilience in vulnerable settings, the polio programme is working to establish a sustainable legacy that will improve health long after global eradication of the virus.
Health workers and community volunteers in remote and security-compromised areas across ten African countries now rely on an SMS-based application to ferret out any possible poliovirus hiding in their midst.
The application is called AVADAR, short for “auto-visual AFP detection and reporting”, with AFP referring to acute flaccid paralysis, which is the main visible clinical symptom of poliomyelitis. AVADAR is an SMS-based mobile application used for reporting, monitoring and surveillance of poliovirus. It was developed in 2016 by the World Health Organization (WHO), in collaboration with the Bill & Melinda Gates Foundation and the Swiss software company Novel-T, to ensure that every case of wild poliovirus is detected.
On a weekly basis, the health workers and volunteers in selected hard-to-reach districts use the AVADAR application to report whether they have noticed any child with paralysis of a limb. The districts are selected based on being deemed high risk yet having the sufficient telecommunications infrastructure that allows the health workers and community volunteers to communicate with the investigations team.
“In the last mile of polio eradication, we are not sparing any resources to reach a polio-free world. That is why we developed the AVADAR app,” says Dr Pascal Mkanda, WHO Regional Coordinator of the Polio Eradication Programme for Africa.
In the WHO African Region, no outbreaks of wild poliovirus have been detected since 2016, when the last case was found in Nigeria’s Borno State. This brings the region closer towards being certified free of wild poliovirus in 2020.
Health workers and community volunteers use AVADAR to recognize and report cases of acute flaccid paralysis, which is the sudden onset of paralysis or weakness in any part of the body that can be caused by polio, among children younger than 15 years. Acute flaccid paralysis could be caused by other diseases than poliomyelitis.
“Polio eradication requires that the surveillance system is sensitive enough to detect all acute flaccid paralysis cases -regardless of the disease behind it- and that such cases are promptly reported and investigated by disease surveillance personnel. This system starts at the community level,” Dr Mkanda adds.
Health workers and community volunteers first received training in workshops on how to use AVADAR and then they were each handed a smartphone with the application installed. On a weekly basis, the app sends them video reminders illustrating acute flaccid paralysis cases. The app then asks: “Have you seen a child with weakness of the legs or arms that you have not previously reported?” They then select between yes or no. If yes, the health workers and community volunteers input extra information about the case, such as the child’s name, date of onset of symptoms and geographic information.
Once the health worker presses the “send” button, a text message is sent to a system that triggers the sending of an SMS to the government and a WHO team that will investigate the case.
“In the AVADAR training workshops, we realized that some health workers and the majority of volunteers do not know the implications of acute flaccid paralysis and are unable to accurately identify such cases within their communities. The weekly AVADAR reminder videos helped improve that significantly,” says Dr Godwin Akpan, WHO Regional Polio Data Manager for Africa.
Dr Godwin is part of the team behind the innovation of the AVADAR application and trains health workers and community members on its use.
AVADAR was first piloted in Nigeria in 2016 and has been rolled out since 2017 in 99 districts of ten African countries: Burkina Faso, Cameroon, Chad, Democratic Republic of the Congo, Liberia, Mali, Niger, Nigeria, Sierra Leone and South Sudan.
As of October 2019, AVADAR has detected 1019 confirmed acute flaccid paralysis cases after health workers and community volunteers sent out 25,747 alerts through the application. None of those cases were polio cases. This marks a significant enhancement to the existing surveillance system that faces difficulties in remote and high-risk areas.
“Innovation and new technologies are our hope to finally make the feat of eradicating polio a reality. Thanks to the Global Polio Eradication Initiative, today, we are closer than ever to eradicating polio,” concludes Dr Mkanda.
In close collaboration with the Bill & Melinda Gates Foundation, WHO’s Regional Office for Africa is continuing to roll-out an innovative disease surveillance platform, enabling the real-time detection of suspected polio cases anywhere on the continent.
Thousands of health workers, volunteers and members of local communities across the continent have been equipped with geo-coded mobile phone technology, and trained to conduct regular and active surveillance visits to health centres across Africa. Professionals and volunteers are tasked to regularly visit local health clinics and actively check for the presence of any child with polio-like symptoms (known as acute flaccid paralysis – AFP), or to look for children in their communities presenting such symptoms. This information is subsequently fed back in real-time to national and regional authorities, enabling for rapid action and immediate dispatch of an investigative team as needed.
“This really is the future of disease surveillance,” comments Reuben Opara Ngofa of WHO’s African Regional Office in Brazzaville, who was instrumental in developing this innovative system and who recently returned from Burkina Faso where he helped roll out the system in remote areas. “Particularly in remote or hard-to-reach areas, we need to know immediately if we have polio circulating in the area, and this system allows for real-time information, which in turn allows for an immediate real-time response. If one of our informants identifies a child with polio-like symptoms anywhere, we will know about it immediately. We are really giving the poliovirus nowhere to run.”
In addition to polio, this system helps detect and respond to other vaccine-preventable diseases, such as measles, yellow fever and neonatal tetanus. Across west Africa, measles vaccination coverage is being assessed through this system, and a cholera outbreak in 2018 in Ethiopia was actively tracked. It is a clear example of the polio infrastructure adding value over and beyond merely eradicating polio.
Thanks to such innovations, and efforts of dedicated professionals and volunteers across Africa, the continent stands on the brink of a historic public health success: the certification of wild poliovirus eradication. In 1996, when Nelson Mandela launched the Kick Polio Out of Africa campaign, wild poliovirus paralysed more than 75,000 children every year, across every African country.
No wild poliovirus has now been detected since 2016, and this real-time GIS surveillance system will provide crucial additional surveillance data, to truly validate the absence of wild poliovirus. Data generated through this system will be critically evaluated by the independent African Regional Certification Committee on polio eradication, when evaluating whether the Region as a whole can be certified as free of wild poliovirus in early 2020.
As the world inches closer towards a polio-free future, finding and closing remaining gaps in national health system capacities to pick up traces of the poliovirus is critical. Only three countries remain on the global endemic list – Afghanistan, Pakistan and Nigeria – but the threat of poliovirus resurgence remains very real, particularly for countries with a history of importation of poliovirus from these endemic areas.
In order to ensure that surveillance systems in these ‘at-risk’ countries are up-to-scratch and sensitive enough to adequately detect and report cases of acute flaccid paralysis (AFP) – a major indicator for polio – the World Health Organization regularly leads expert reviews to put systems under the microscope.
Expert review in Sudan
Eighteen technical officers and polio surveillance experts from WHO, UNICEF, the U.S. Centers for Disease Control and Prevention, the Bill & Melinda Gates Foundation and the Eastern Mediterranean Public Health Network recently met with Ministry of Health staff in Khartoum to share their findings and recommendations after scrutinizing Sudan’s surveillance performance at federal and state levels.
“Sudan has not seen a case of polio for almost nine years, however, certain factors put it at considerable risk of poliovirus importation and outbreaks,” said Dr Naeema Al Gasseer, WHO Representative to Sudan. “It is very important that the country remains on guard against polio and continually analyses and improves the quality of its AFP surveillance, particularly in the high risk areas,” she said.
“Strong AFP surveillance is a cornerstone of the polio eradication effort ̶ it enables us to quickly pick up poliovirus if it is circulating and react with an appropriate response,” said Dr Ni’ma Abid, a senior technical expert from WHO’s regional polio eradication hub in Amman, Jordan. “There is no margin for error and in at-risk countries facing such challenges as Sudan, we need to thoroughly examine AFP surveillance systems to make sure that they are sensitive and fast enough to detect transmission. This is a practice that will need to continue even after the world is certified polio-free,” he added.
Risk factors and special strategies
Sudan is the third largest country in Africa and home to over 40 million people. Insecurity, forced displacement, frequent nomadic population movement and inaccessibility in some areas make it challenging for health workers to consistently reach all children with vaccines to build immunity. Refugee influxes across porous borders with conflict-affected neighbouring countries exacerbate the risk of disease and compound pressures on the country’s already stretched health system. In addition, high sub-Saharan temperatures and rough expansive terrain can make timely collection and transportation of stool specimens from children with AFP for laboratory testing difficult.
Special strategies have been devised to cater for the specific surveillance challenges associated with reaching high risk groups. Examples include active searches for AFP cases and sample collection by community-based surveillance officers in areas with access issues, the mapping of the movement of displaced populations, and establishing regular communication with nomadic community focal points who report AFP cases via mobile phone. In refugee camps, vaccination posts have provided an opportunity to screen for children with AFP, and collaboration and sensitization of non-government organization (NGO) staff has helped to improve reporting of AFP cases.
Eighteen states were assessed throughout the review, with visits to 90 health facilities, the families of 16 children with AFP, and high-risk special populations. Overall conclusions were that the system is meeting global AFP surveillance targets and it is unlikely for polio to circulate undetected. However, gaps were identified that need to be addressed.
“Surveillance system performance in Sudan is sensitive and we were pleased to see implementation of the recommendations made at the last review,” said Dr Abid. “However, more attention needs to be paid to surveillance in refugee communities, cross-border population movement, and programmatic issues such as the high level of turnover of national surveillance staff,” he said. “We encourage the government of Sudan to implement the recommendations made at the review to address these and other gaps,” he said.
“WHO and partners commend the government of Sudan for its efforts to date, and stand ready to advise and support to keep the country polio-free,” said Dr Al Gasseer. “Until polio is gone for good, globally, we must make every endeavor to prevent resurgence,” she said.
Sudan witnessed its last case of indigenous wild poliovirus in 2001. Since then it has been exposed to several wild polio importations from Chad and Ethiopia with its most recent case in March 2009.
A child in west Africa receives polio vaccine. Photo: WHO.
More than 190 000 polio vaccinators in 13 countries across west and central Africa will immunize over 116 million children over the next week, to tackle the last remaining stronghold of polio on the continent.
The synchronized vaccination campaign, one of the largest of its kind ever implemented in Africa, is part of urgent measures to permanently stop polio on the continent. All children under five years of age in the 13 countries – Benin, Cameroon, Central African Republic, Chad, Côte d’Ivoire, Democratic Republic of Congo, Guinea, Liberia, Mali, Mauritania, Niger, Nigeria and Sierra Leone – will be simultaneously immunized in a coordinated effort to raise childhood immunity to polio across the continent. In August 2016, four children were paralysed by the disease in security-compromised areas in Borno state, north-eastern Nigeria, widely considered to be the only place on the continent where the virus maintains its grip.
“Twenty years ago, Nelson Mandela launched the pan-African ‘Kick Polio Out of Africa’ campaign,” said Dr Matshidiso Moeti, WHO Regional Director for Africa. “At that time, every single country on the continent was endemic to polio, and every year, more than 75 000 children were paralysed for life by this terrible disease. Thanks to the dedication of governments, communities, parents and health workers, this disease is now beaten back to this final reservoir.”
Dr Moeti cautioned, however, that progress was fragile, given the epidemic-prone nature of the virus. Although confined to a comparatively small region of the continent, experts warned that the virus could easily spread to under-protected areas of neighbouring countries. That is why regional public health ministers from five Lake Chad Basin countries – Cameroon, Central African Republic, Chad, Niger and Nigeria – declared the outbreak a regional public health emergency and have committed to multiple synchronized immunization campaigns.
UNICEF Regional Director for West and Central Africa, Ms Marie-Pierre Poirier, stated that with the strong commitment of Africa’s leaders, there was confidence that this last remaining polio reservoir could be wiped out, hereby protecting all future generations of African children from the crippling effects of this disease once and for all. “Polio eradication will be an unparalleled victory, which will not only save all future generations of children from the grip of a disease that is entirely preventable – but will show the world what Africa can do when it unites behind a common goal.”
To stop the potentially dangerous spread of the disease as soon as possible, volunteers will deliver bivalent oral polio vaccine (bOPV) to every house across all cities, towns and villages of the 13 countries. To succeed, this army of volunteers and health workers will work up to 12 hours per day, travelling on foot or bicycle, in often stifling humidity and temperatures in excess of 40°C. Each vaccination team will carry the vaccine in special carrier bags, filled with ice packs to ensure the vaccine remains below the required 8°C.
“This extraordinary coordinated response is precisely what is needed to stop this polio outbreak,” said Michael K McGovern, Chair of Rotary’s International PolioPlus Committee . “Every aspect of civil society in these African countries is coming together, every community, every parent and every community leader, to achieve one common goal: to protect their children from life-long paralysis caused by this deadly disease.”
The full engagement of political and community leaders at every level – right down to the district – is considered critical to the success of the campaign. It is only through the full participation of this leadership that all sectors of civil society are mobilized to ensure every child is reached.
US$ 22 million urgently needed for outbreak response in Congo — appeal from WHO, UNICEF and Rotary International.
A child is immunized against wild poliovirus in Luanda, Angola, in October. The Republic of Congo is now tackling an explosive outbreak of wild poliovirus that is genetically related to virus that had been circulating in Angola. Melissa Corkum/UNICEF
As of 7 December, at least 476 cases of acute flaccid paralysis (AFP) and 179 deaths have been reported from the site of the acute poliomyelitis outbreak centred in Pointe Noire, Republic of Congo. Six cases have been confirmed to have been caused by wild poliovirus type 1 and laboratory testing continues. Initial data indicates the majority of the reported cases and deaths involve young adults aged 15-25 years. Nearly all cases have been reported from the port city of Pointe Noire, with cases also reported from Niari, Bouenza, Brazzaville, and Kouilou. New cases continue to be reported.
Genetic sequencing of the poliovirus detected has determined that the polio cases are caused by a poliovirus most closely related to that circulating in neighbouring Angola. Congo had recorded its last case of indigenous polio in 2000.
Significance and Risks:
Stopping the outbreak in Congo is a top international public health priority due to the explosive, deadly nature of the outbreak and the high risk of further national and international spread. As well, given that polio is a disease slated for global eradication and the recent progress in Nigeria (98% reduction in cases in 2010 compared to the same period in 2009), rapidly stopping the persistent poliovirus transmission in central Africa (i.e. Angola, DR Congo) and stopping new polio outbreaks such as in Congo, are of critical importance.
The outbreak in Congo is worse than other recent outbreaks of polio due to the extraordinarily high mortality rate seen so far and its explosive nature, with the poliovirus rapidly circulating through a susceptible population. Despite this, experience from other either explosive or adult outbreaks (ex. Namibia, 2006) demonstrates that it can be rapidly controlled if we have the necessary funds to respond appropriately with swift, high-quality vaccination activities. The speed of the outbreak response is vital to stopping the further spread of disease.
Regional Emergency Outbreak Response Activities:
Three elements are central to quickly stopping this outbreak, per the World Health Assembly resolution of 2006: immediate, mass oral polio vaccine (OPV) campaigns with the appropriate type-specific vaccine (a minimum of three such campaigns, and based on other, similar outbreaks, up to eight campaigns, two to four weeks apart); mass OPV campaigns in bordering areas; heightened AFP surveillance in the country and neighbouring areas. The response to the outbreak in Congo also includes all the new innovative emergency response approaches, including the new short interval additional doses (SIAD) strategy, which has increasingly proven to more rapidly stop outbreaks and prevent international spread. Finally, heightened surveillance must be sustained for more than 12 months to ensure that the outbreak has stopped and to guide further actions. Conducting this type of response, though, requires rapidly mobilizing emergency funds.
The Government of Congo has alerted the public to the outbreak and launched an emergency response plan, with support from key partners, including WHO, UNICEF, Rotary International and the US Centers for Disease Control and Prevention (CDC). The first vaccination response, using monovalent oral polio vaccine type 1 (mOPV1), was launched by the First Lady of Congo and the Minister of Health on Friday, 12 November, in Pointe Noire and targeted 1.3 million people of all ages and covering the whole population of Porte Noire and Kouilou, in conjunction with the neighbouring province of Cabinda in Angola and 16 districts in the neighbouring province in DRC. The remainder of the country (target: approximately 3 million) conducted sub-national immunization days with mOPV1 from 18-22 November, which were launched in Brazzaville by the Head of State.
A second nationwide round took place starting 3 December and a third nation-wide round is scheduled for 11 January. Parts of DRC and Angola will also be covered during these rounds, and other neighbouring areas will be monitored and response mobilised as necessary. While full coverage data from the first two rounds is still be analyzed, early indications are that both campaigns were of good quality, with approximately 105% of the target population reached during the first round. As importantly, key lessons learned from the first round were immediately integrated into planning for the second round. These include strengthening the ‘fixed post’ immunization outreach, to facilitate reaching an adult population which may not be at home during house-to-house vaccinations conducted during the day.
The number, geographic extent and target age groups of further campaigns will be determined by the Government based on the evolving epidemiology. The multi-country campaign may be further expanded to cover additional bordering at-risk areas.
Countries across central Africa should strengthen AFP surveillance to rapidly detect any poliovirus importations and facilitate a rapid response. Countries should also address any gaps in polio immunization coverage to minimize the consequences of a poliovirus introduction. As per the recommendations in the WHO publication International Travel and Health to and from all countries where polio is circulating, including the Republic of Congo and Angola, should be fully protected by vaccination.
Funding is urgently needed to ensure emergency response activities can take place. To date, US$6.2 million has been confirmed or is tentative, leaving a funding gap of US$ 15.7 million.
There are five major components of the Global Polio Eradication Initiative budget:
1. Oral polio vaccine supply
In 2009 alone, 2.2 billion doses of vaccine were used to vaccinate children as part of polio eradication efforts. Vaccines are procured by UNICEF. The agency works to ensure that the vaccine supply is secure – with multiple suppliers – and that the price is both affordable for purchase and reasonably covers the needs of the manufacturers.
2. Operational cost of supplementary immunization activities
Supplementary immunization activities are vast operations to deliver vaccine to every household. Detailed maps and plans have to be updated for every dwelling in the area to be covered, vaccines have to be delivered to distribution centres, and vaccinators need to be trained to visit every household and vaccinate every child.
3. Social mobilization and communication:
Experience has shown that it is critical to have strong social mobilization and communication activities planned and implemented prior to immunization campaigns. This requires development of communication plans, involvement of the community leaders and civil societies as well as mass media. Such activities ensure community awareness about the outbreak, planned response and targeted age group. It also secures acceptance to the vaccination efforts and has impact on coverage as community members are mobilized to ensure the targeted age groups are being vaccinated during the each and every round.
4. Surveillance
Surveillance budgets cover the detection and reporting of acute flaccid paralysis (AFP) cases. This is done through an extensive informant network of people who first report cases, and through active searches in health facilities.
5. Technical assistance
When relevant skills are not available within a national health system, staff and consultants are sent to fill the gaps. This extra support helps with immunization campaign planning and implementation, logistics, forecasting and supply management, human resources, communication and social mobilization. Polio eradication staff now constitute the single largest resource of technical assistance for immunization in low-income countries.